Transcript Society for Maintaining Integrity on The Earth Inaugural Meeting Opening Remarks and Keynote Address
Good morning. I’m Michael, the Chair of the Ethics Department at the Society for Maintaining Integrity on The Earth and I’d like to welcome you to this inaugural meeting. It’s good to see all of you who accepted our invitation, and I’m looking forward to meeting with all of you individually. These are exciting times for all of us as we embark on this new project.
I’d also like to introduce Peter, our database administrator and technical wizard. Say hello, Peter. (Peter smiles, waves, and mumbles a greeting.) Peter will be leading the afternoon computer training workshop. He will also introduce the new phone app for Android and iPhone. This allows much faster access to information you’ll need to assess any situation. We haven’t yet activated the function because we still want you allow time for deep contemplation before acting.
A few housekeeping items before we get started. Lunch will be from 11:30 am until 1:00 pm in the Grand Ballroom. Be sure to bring the tickets that are behind your name badges. A bus for your spouses’ slash significant others’ activities will leave from the main entrance at 1:15pm and return in time for dinner.
Joseph Stalin famously said, “Everyone has the right to be stupid, but some people abuse the privilege.” I’ve been active since the first Homo sapiens appeared, weeding out those whose excessive stupidity threatened humanity’s survival and progress. Sometimes it was so rampant that I’m amazed you’ve accomplished anything in the past ten thousand years.
My job was much simpler in prehistoric times. There were fewer people and natural selection – what you call Darwinism – was very efficient. If you were persistently stupid, some ferocious beast decided you might make a nice snack (with a little subliminal suggestion from yours truly). Irritating the rest of the tribe might get you thrown into a volcano, justified by the flimsy excuse of “appeasing the gods.”
Now and then Administration had to periodically step in and thin the herd. Destroying almost everyone and everything with The Great Flood was regrettable, but that instilled the fear of The Almighty in the survivors, at least for a few centuries.
Later I experimented in Ancient Egypt, using the more articulate among the masses – Moses, David and others – to provide blatant warnings. The Pharaoh got nine warnings before the smiting began. I think DeMille’s casting of Yul Brynner was genius and I must admit a certain fondness for that stunt with the Red Sea.
A millennium and a half later, Administration had a great idea. Why not send Himself to live among the people? You recall how well THAT worked out. After the Resurrection the stupid in power – it’s amazing how the latter attracts the former – treated the disciples rather badly. Even a well-written manual wasn’t good enough for some – yes, I realize men don’t like to follow instructions – but then using it to inflict unspeakable pain has been humanity’s most despicable perversion.
Earthquakes, fires, the Black Death – all managed to keep the great unwashed under some control. That is, until things improved over the next couple of centuries and people began throwing caution to the wind. We found ourselves back at square one. The Renaissance was but a brief respite from idiocy. Humanity been remarkably resistant to guidance and reason.
By the twentieth century I had to become less subtle in my messages. That guy on the street, the one dressed in rags who held the sign that said, “The End is Near?” He wasn’t crazy; he was a walking Public Service Announcement. Targeted individuals who noticed but ignored the obvious hint later met with an unfortunate “accident.”
But the burgeoning population made it difficult for me to keep up with the workload. Social media has brought out the worst in people and you can thank those media czars for record levels of stupidity. Administration decided I needed some help, and that is where you come in.
You’ve all been selected for various reasons, for the Lord works in mysterious ways. Some of the people close to you probably wondered, “Why him (or her) and not me? I could do a damn good job of smiting!” We appreciated their enthusiasm but there’s more to it than just summarily dispatching everyone who irritates the crap out of you. One of this morning’s sessions will cover the guidelines for choosing those most deserving. Our next session will discuss why you were chosen.
Thank you for attending and I hope you all find these talks illuminating.
WARNING: This post contains material of a sensitive and sexual nature. If you are easily embarrassed or squeamish, you might want to sit this one out.
I saw the Urology Department Physician Assistant the week after my surgery to take out my catheter. She gave me a prescription for 50mg sildenafil (generic Viagra) tablets and told me to take a half tablet every night “to keep the blood flowing” – a prophylactic Roto-Rooter®. I made an appointment with her and the Vacuum Erection Device Clinic for January as “the December clinic had already passed.” I was supposed to talk with the clinic about acquiring a “medically approved” vacuum erection device in January, but I pushed to get it ordered in December since they run upwards of three hundred bucks and I’d met my deductible for the year.
I got a mysterious text message from FedEx alerting me to a delivery from upcrx.com that required my signature. Often “signature required” means either someone is sending alcohol, or the IRS wants to do an audit. Google helped me find University Compounding Pharmacy in San Diego but did nothing to alleviate my confusion.
The package arrived the following week. I scrawled my name on the driver’s tablet and I now possessed my very own prescription “Austin Powers Swedish Penis Enlarger.” I wasn’t supposed to use it until after my postoperative appointment in January, and then only “under medical supervision,” lest I somehow injure myself.
I had an appointment in January with Dr. Fine for a postoperative visit. The PSA level I’d had drawn the previous week was undetectable; I’d get a PSA level done every three months for a year, then every six months if all went well.
He asked about my recovery.
“It’s going fine. The big incision burned every time I moved but that went away in a week and I used the Norco maybe three times. I got by on Tylenol. And I’m back to my pre-surgical level of incontinence.”
His eyes lit up!
“You should really see one of the pelvic physical therapists. There are a couple of people who specialize in male incontinence therapy.”
“I’m fine.”
“You really should consider it; nip it in the bud right now.”
(Like I have the time or inclination to have some dude teach me Kegel exercises, which I’d taught women for decades.)
“Ok, I’ll give them a call.” (No, I won’t.)
Many physicians are hardwired to offer as many labs, procedures, and referrals as possible. That is probably why sleep studies have been such a standard for anyone who is fat, diabetic, hypertensive, and/or chronically tired. He gave me the phone number which I tossed into the trash on my way to the car.
It’s been seven months since surgery; I don’t wear underwear shields anymore and the urgency is almost nonexistent. I may not be able to write my name in the snow but it no longer feels like I’m trying to urinate through a urethra in a death grip.
The following week I saw the P.A. She had asked me to come in early because she had to go somewhere. Today she was a little frantic and hurried through her instructions.
“You’ll be talking to Jonathan about the vacuum. Stop taking the Viagra while you are using it. Try the Viagra after a couple of weeks. If you don’t see any results after several tries, it’s time to open this little white bag and take the pill that’s in there. If you’re still not getting any results after 2 months, you need to come see me. Here’s an instruction sheet. Now I have to go…”
My next stop was the pretentiously named Vacuum Erection Device Clinic. I figured I’d be in a classroom with several other men discussing our surgical recovery, led by a physician in the requisite white coat giving us a talk on the mechanism of tumescence and how our recent surgery had interfered with function.
Instead, I went to another room and met with the “physician liaison” (read: equipment rep).
“I’ll need to order your device and when it comes in, we can talk about how to use it.”
“Uh, I got it last month.”
“Ok, then. Here’s what you do. Put it over your penis. Pump the vacuum for five or ten seconds, then wait forty-five seconds. Release the vacuum, wait a minute, and then pump it again for five to ten seconds and wait forty-five seconds. Do that for 10 minutes a day. If you have any questions, here’s my card.”
I wasted an afternoon for this?
How an erection works.
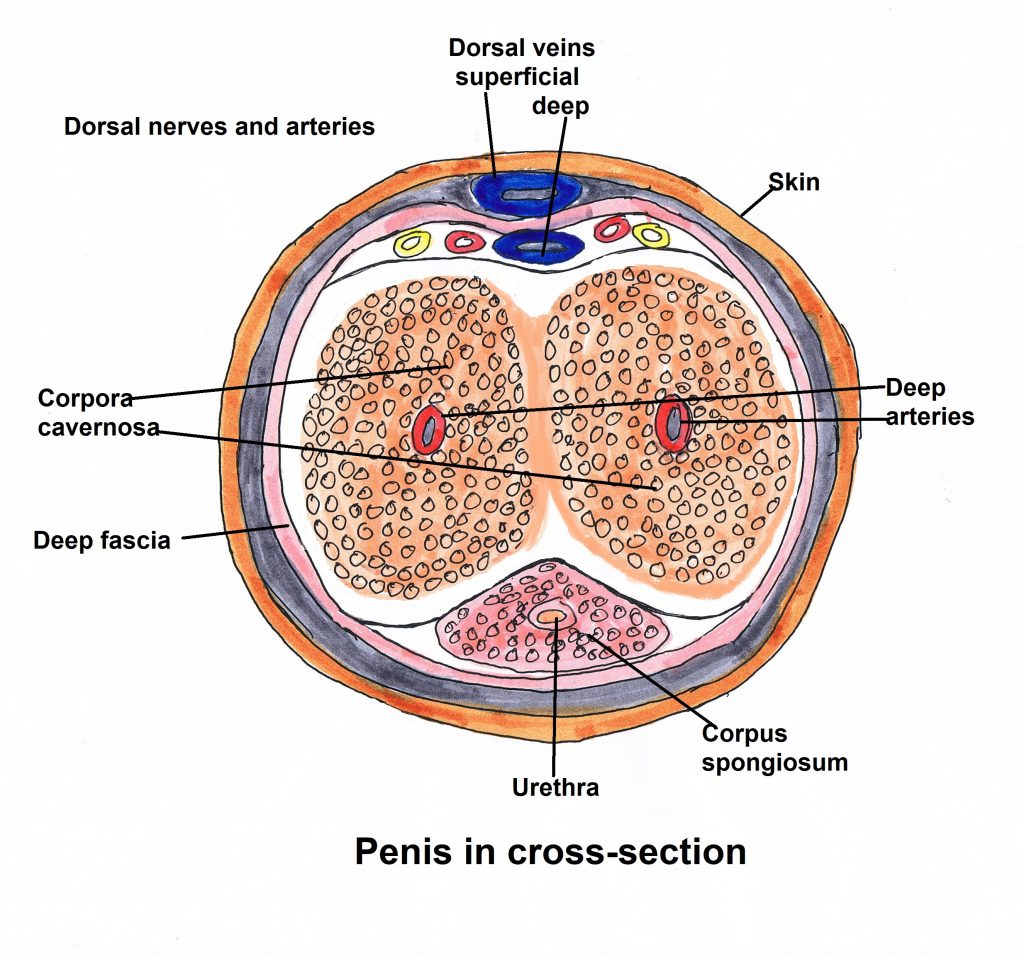
The cross-section of the penis looks like a cartoon monkey face. The shaft of the penis contains two spongy cylinders, the corpus cavernosum; a sizeable artery runs through each. A vein flanked on each side by an artery and a nerve runs above the corpus cavernosum. All this is surrounded by a layer of fascia, like a hot dog casing. A third spongy tube, the corpus spongiosum, surrounds the urethra and runs the length of the shaft below the corpus cavernosum while the dorsal penile vein runs the length of the shaft on top. All this is enclosed in loose tissue and covered by thin, flexible skin.
The arteries in the corpus cavernosum normally aren’t fully open, which is why men don’t have permanent erections. When the brain is stimulated, a combination of nerve impulses and chemical signals open the arteries which fill the corpus cavernosum with blood. The engorged tissue presses on the veins, blocking return blood flow and, voilà, an erection is born.
It’s been suggested that men hit their sexual peaks at 18 and it’s downhill after that. Research, however, shows men’s testosterone levels peak in their 30s before gradually declining. Getting an embarrassing, spontaneous erection for no apparent reason disappeared by my late teens. Sexual function can decline as early as one’s 40s; I started noticing a difference in my late 40s. Other things can affect sexual drive and function besides purely aging:
medical conditions (diabetes, high blood pressure, heart disease, obesity, depression)
certain medications (blood pressure medications, antidepressants, narcotics and others)
Bad habits (excessive alcohol consumption, smoking, recreational drugs, lack of sleep)
The nerve bundles required for achieving an erection are often damaged during a radical prostatectomy. Scarring around my prostate required taking out the neurovascular bundle on the right side. The left side was spared but the trauma from surgery is enough to keep the remaining nerves from doing their job. It may take up to two years before being able to achieve an erection with or without ED drugs. If that doesn’t work, the alternatives are injections into the penis or penile implants.
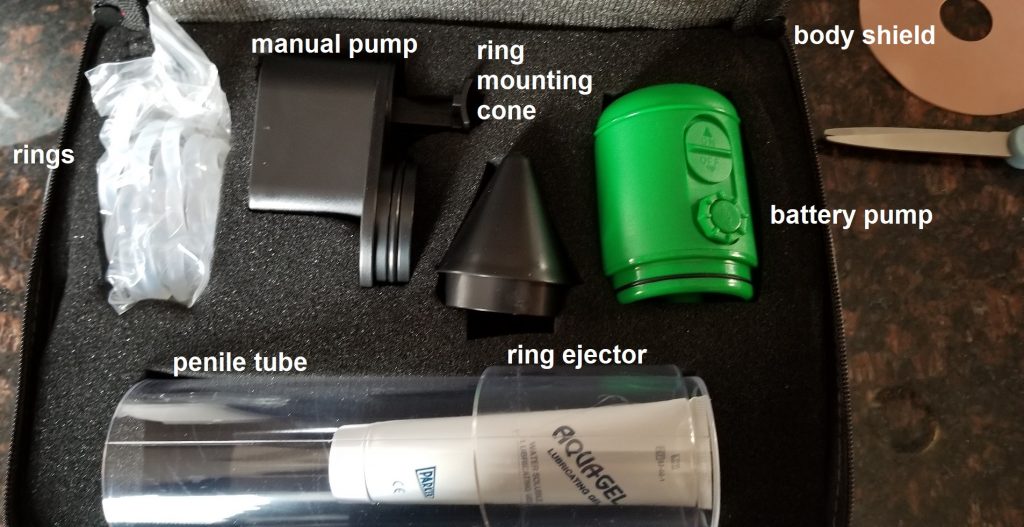
This is my device. It has both battery-operated and manual vacuum pumps which attach to an acrylic cylinder. There are five silicone rings (sizes 5 to 9); the cone is used to slip a ring onto the other end of the cylinder. The ring ejector twists to push the ring onto the penis before removing the cylinder to maintain the erection. The body shield is that circular thing resembling a old-fashioned floppy disk drive and provides a barrier to prevent scrotal skin from being sucked into the pump. The gel is used to form a seal around the base of the pump and to lubricate the penis; without it the penis will drag along the cylinder wall like an anchor on concrete.
Note to self: make sure to grab the correct white squeeze tube: the lubricating gel tube, not the menthol gel I use on sore muscles.
The Vacuum Erection Device, aka the “Austin Powers Swedish Penis Enlarger”
The caveats in the instruction manual were disturbing.
“Vacuum therapy may cause a small “blood blister” on the head of your penis. This is normal and not harmful.”
“The rings may bruise the base of your penis. Some bruising is normal and should not be cause for alarm.”
Wait, what? In what alternative universe is a bruised and blistered penis “normal?”
“If you wear a ring for more than 30 minutes, you may severely bruise or damage your penis.”
So, if that happens, do I just get a new one from Amazon with 2-day Prime delivery?
I looked over the instruction sheet I’d gotten from the P.A.
You were given samples of ED medication to try at your leisure. Please use the paper form you were given (to) track your response and side effects of each medication. The goal is for you to try one tablet every 3rd day followed by (significant) stimulation.
Tablets work better on an empty stomach
Tablets take one hour to become effective
Space out your trials by 2-3 days at the minimum
If tablets do not work, you may still have intercourse with the vacuum rubber bands.
Common side effects – headache, facial flushing, nasal congestion
If you are on Cialis and are experiencing leg cramps – Please stop Cialis immediately as Cialis can sometimes be linked to tendon inflammation, possible rupture.
Oh, goody!
I discovered the vacuum doesn’t work immediately, which was disappointing. One cannot hope to instantly inflate the penis like a balloon that a clown twists into animal shapes for kids at a party. At first it took fifteen minutes to achieve anything resembling an erection, which decreased to around five minutes after three months. The least they could do is make pumps entertaining with indicator lights and an alarm that goes off when one has reached maximum height (or is it length?).
Anyone who played with a vacuum cleaner hose as a kid knows it can inflict some pain if left on a body part for too long. Moving blood into a penis with negative pressure is an uncomfortable process and certainly not erotic. And few things are worse than having a large chunk of scrotal tissue suddenly sucked into the cylinder along with a testicle. The barrier did not help at all; it was too flexible and got drawn in as well.
It didn’t take long for one of the rings to break and the replacements cost twenty bucks each. I ordered a different kind of ring that looked like a flat, silicone bagel (the penis goes through the hole and the surrounding material blocks wandering skin, but it was for a rival brand and didn’t fit my pump. I found another type that looked more like a foam-lined chip clip (or a cigar cutter). I settled on a silicone loop I bought from Amazon.
The battery pump died after a month. The company said they’d send a replacement which never arrived, and I don’t feel like calling them again. The manual pump is equally effective but using it leads to spasms in my right thumb and pain in my right wrist, caused by old nerve damage from two separate lacerations. The recommended forty-five seconds on, one minute off did nothing, even after multiple attempts over three weeks. I finally just pumped and left the vacuum on for several minutes while amusing myself with my Kindle game. (I may not have sexual function, but at least I’m doing my part to delay age-related dementia!) My erections promptly deflated as soon as I released the vacuum, despite the ring. There was never sufficient rigidity to close off the penile veins.
I then tried using 100mg sildenafil without the pump or any kind of stimulation. I got a slight flush but nothing. A few days later I made another attempt. I got distracted doing other things but applied the pump three hours after I took it. I got a reasonable erection which again deflated after taking off the pump and using the loop. I tried the pump again and then manual stimulation which made it last a little longer but still wasn’t anything to write home about. And all this took about 25 minutes, not including the minimum one hour wait for the drug to take effect.
George Burns said, ““Sex at age 90 is like trying to shoot pool with a rope.”
But all is not lost. Men can have orgasms without an erection, although it may take some mental adjustment. If you’re a New Ager into Tantra (and you have a lot of patience), you can have an orgasm using just your mind. Radical prostatectomy removes the prostate and seminal vesicles, meaning there’s no more semen, along with the sphincter between the urethra and the prostate, which normally prevents retrograde ejaculation (semen going into the bladder instead of out the penis). The result is climacturia, the release of urine with orgasm and a common side effect of the surgery. One can prevent this with an adjustable loop around the penis, muscle training or surgery, but emptying the bladder beforehand is the simplest.
More information than you ever wanted to know, eh?
Finally, nothing is more important during post-prostatectomy rehabilitation than a loving and supportive partner. Peg says she would rather have me alive and annoying than six feet under, and for that I am grateful.
It’s a good thing Dr. Fine’s reputation preceded him, or I might not have stayed long enough to meet him. But first, a segue into the genesis of my ire.
When Corporate America took over health care administration, it decided physicians had wasted too much time taking care of patients instead of generating revenue. Large health care organizations began buying up individual physician practices and, in some cases, taking over hospitals. Younger physicians loved this idea: they got a salary, paid vacation and none of the administrative hassles of running a private practice. (I plead guilty, as I joined an HMO for those reasons. I was a poor businessman and I admitted it. The problem was, in many cases, I knew more about business principles than the people signing my paychecks.)
Older physicians balked at being controlled and some of them resisted as long as they could. If you didn’t play ball, The Corporation would find ways to shut you out. If you didn’t contract with the predominant insurers, you became “out of network” and a lot more costly to patients. Other older physicians saw the handwriting on the wall and retired early, the lucky bastards, to stay at home, engage in hobbies, travel or annoy the wife full-time.
We traded autonomy for financial security and ended up with neither.
The Corporation now controlled everything, including your ass, so it could dictate how you did your job. One physician I knew 25 years ago, a hospital employee, said, “I have guys in three-piece suits telling me what to do. And I do it.” Thus, the standard 10-minute appointment was created. No matter how complex the patient, physicians were expected interview, examine, diagnose and treat a patient in the allotted time before moving onto the next one. Or should I say “mooving on”, since patients were now herded through like cattle. (I often threatened to play the Rawhide theme in the hallway during my HMO days. “Head ‘em up! Move ‘em out!”)
If you were a specialist, you got 20 or 30 minutes for consults, even if the patient had cancer. No “wasting time,” like my gyn oncology professor during residency, who spent an hour discussing ovarian, uterine or cervical cancer with women who were still in shock from the diagnosis.
And now, back to our regularly scheduled blog post.
Dr. Fine’s office booked a 30-minute visit at 2:50 p.m. Peg and I arrived about 15 minutes early; she was still in a wheelchair after having foot surgery. I checked in, sat down and waited. And waited. And waited.
About 40 minutes later a nurse, nursing assistant or whatever, appeared in the door to the inner sanctum and bellowed, “David.” I got up and wheeled Peg through the open door.
Halfway down the hall, the nurse said, “David, what is your date of birth.”
I told her and she said, “Oh, wrong David.” So, I wheeled Peg back to the waiting room while the correct David was whisked away.
Twenty minutes later she reappeared. “David.” Once again, I wheeled Peg down the hallway, but not as far this time before she realized my date of birth didn’t match what was on her tablet. And, once again, I wheeled a now pissed-off Peg back to the waiting room.
Different women appeared at the magic door, calling names as if they worked in a cheap restaurant, and patients disappeared.
It was now 4:15 pm. I’m normally a quiet, patient type (you shaddap and stop laughing!), but even my patience was wearing thin. The first woman we saw opened the door and called, “David.” “Which one?” “Last name Rivera?” “Yeah, that’s me.”
We were herded into a pen patient room and a few minutes later a very sweet assistant came in to verify my information on the computer terminal (paper charts have all but disappeared). She apologized for the wait and said Dr. Fine would see us soon, but he was running behind.
Peg smiled but said, “We’ve been waiting a long time. Dr. Fine better be a rock star!”
The SYT swallowed and assured us Dr. Fine was indeed was, figuratively speaking, on par with Jimmy Page.
We could hear snippets of Dr. Fine’s conversation with another patient. Another 15 minutes elapsed, then yet another nurse/assistant came in with two books. I don’t recall the titles, but they could be titled, “You and Your Prostate,” and “What You Need to Know about Prostate Cancer.”
“The doctor will be in shortly to discuss your diagnosis.”
Now I was pissed! “I’m a physician! I KNOW my diagnosis; Dr. Ky and I have talked about it and I’m here to talk about getting a surgery date scheduled!” I thought If you’d looked at the record before barging in here, you’d know what’s happened and why I’m here.”
Finally, Dr. Fine entered the room and I understood why he was running late. He greeted us and apologized for running late. “Discussing a new diagnosis of cancer with a patient takes some time and I don’t want them to feel rushed.”
Ok, you earned your rock star status.
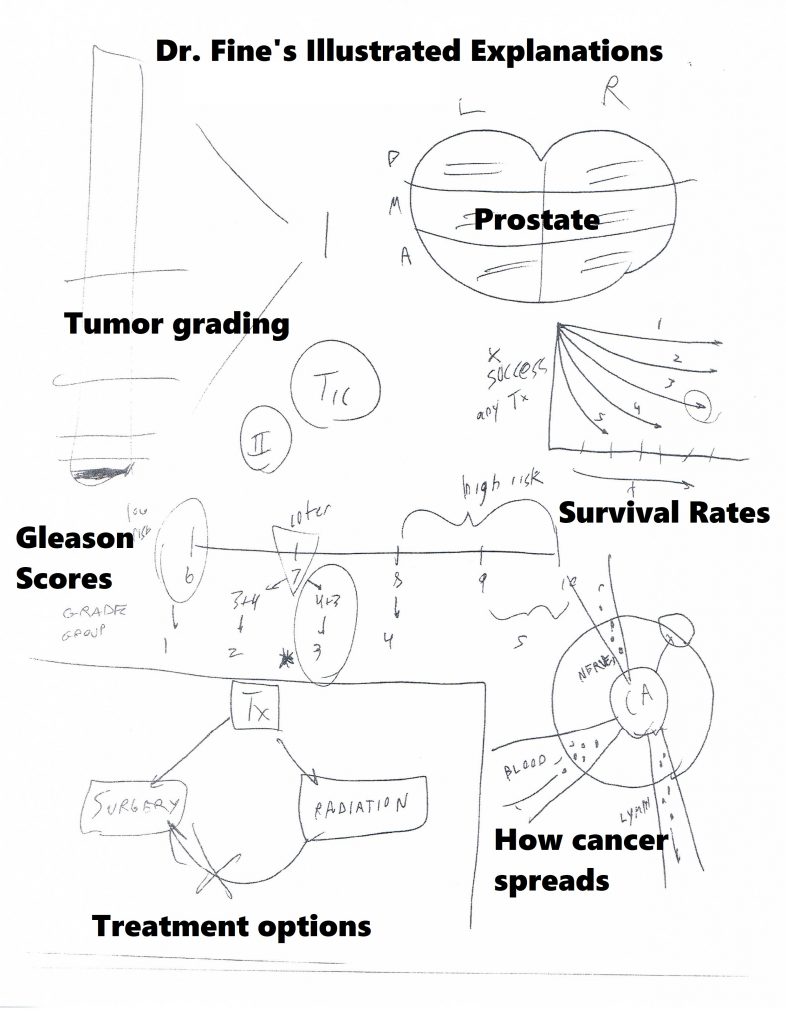
He talked at length about Gleason scoring in general. A Gleason score of 6 suggests one’s cancer is likely to grow slowly while a score of 8 and above is likely to be more aggressive and spread quickly. My score of 7 (4+3) put me at intermediate risk and was more concerning than a score of 3+4. Then he talked about Tumor, Node and Metastasis (TNM) staging and how that relates to overall survival; my cancer stage was T-IIa, meaning no metastases or node involvement. (For more information, go to the Urology Care Foundation educational materials page and download the Localized Prostate Cancer guide.)
Notes from our discussion of prostate cancer and treatment options
We then discussed treatment approaches. I talked about the risks of radiation in my previous post, but the biggest drawback is it turns the prostate to mush. If the cancer recurs, taking out the prostate is next to impossible. Doing surgery first leaves radiation as an option for recurrence.
Surgery removes the prostate completely and, potentially, all of the cancer, but has its own set of risks. Immediate problems include recovering from surgery, including having a catheter in one’s bladder for a week. The surgeon has to cut the urethra (that tube from the bladder to the outside) to remove the prostate, and then sew it back together. One is likely experience some degree of urinary incontinence once the catheter comes out; they recommended getting a large supply of “adult incontinence underwear” along with pads that look like what women wear after delivering a baby.
Surgery removes the seminal vesicles and potentially some nerves along with the prostate, guaranteeing temporary or permanent erectile dysfunction. I would be taking a low dose of the “little blue pill” (sildenafil) every day to “promote blood flow” back into a limp penis. I’d have a checkup six weeks after surgery and then go to the Austin Powers Swedish Penis Enlarger clinic to learn how to use a $300 “medical grade” acrylic cylinder and vacuum pump. For some reason they discourage procuring the much cheaper products available at your friendly neighborhood adult toy store as it could “result in injury.” (Like Ralphie getting his tongue stuck to the frozen flagpole in “A Christmas Story?”)
We agreed to a surgery date right after Thanksgiving. He gave me a card for the Patient Navigator, someone who is supposed to “guide you through the process.” I talked with her once; she told me someone from the hospital “will call you with a surgery date within a couple of weeks. Then someone will call you a week before surgery with questions and instructions.” I used to impart that information to my patients at the end of our visit and didn’t need someone to do it for me.
I saw one of the Urology Department P.A.s (physician assistant) to teach me Kegel exercises, which help control the inevitable leaking bladder after surgery. Women learn Kegels when they are far younger, since they have only one urethral sphincter to men’s three. I told her I’d been wearing protection for months to which she replied, “Welcome to our world.” The visit lasted only a few minutes. Peg had taught me abdominal core and Kegel exercises to do while driving to client’s houses. She did a better job and for free.
About a week later someone from the hospital’s scheduling department called me while I was driving to a client’s house. My surgery would be on December 2 at 7:30 a.m., a wretched time, as I’d have to be there about 2 hours earlier for preparation (which often takes about 30 minutes).
“I’m wandering around the Chicago suburbs so now isn’t a great time to talk. How about you give me a call next Monday when I’m home?”
“Ok, that would be fine. In the meantime, I’ll send you preoperative instructions through our website and we can go over them next week.”
She called and went over my medical history – current and past illnesses; the medications I took; allergies to medications – before going over the same instructions she’d sent the week before. I realize it may seem redundant, but there are people handicapped by a Y chromosome who don’t read or listen and need all the reinforcement they can get.
“Back in the good old days, I used to do all this myself.” She replied, “You probably weren’t that busy back then.”
Bullshit. I routinely saw 25-30 patients a day in the office and worked in women with acute problems. I did my own preop H&Ps (history and physical) and dictated it on the hospital’s transcription line. Years later, wrote my reports in MS Word and hand delivered them to avoid hearing, “We can’t find your H&P. Did you forget to dictate it?”
Preparing for surgery
Physicians go through “informed consent” with a patient before surgery or a significant treatment. Ideally, a physician explains what s/he proposes doing, what it is meant to accomplish, the risks and benefits of the procedure (including risk of death, if appropriate), and what might happen if the patient refuses. Then the physician gives the patient time to ask questions, have those questioned answered and, often at the end, sign a permit for said treatment or surgery.
This ritual is supposed to ensure the patient makes a well-informed, intelligent decision while also minimizing the risk of litigation in the event of an adverse occurrence or outcome. In reality, a pissed-off patient can always claim “I didn’t know what I was agreeing to” and some lawyer will take the case. So, many of us believe there is no such thing as truly “informed consent.”
My approach to informed consent for surgery went something like this:
“You need to be at the hospital two hours before your surgery time. They will get you ready for surgery (but it doesn’t take two hours, so you’ll spend a lot of time picking your butt). When everyone is ready, one of the nurses will take you to the operating room, put you on the table, hook up EKG leads and strap you down, so you don’t roll off. (Sometimes we will pick our butts waiting for anesthesia to stroll in.) I will be there before you go to sleep. This procedure is going to take about x hours. You’ll go to the recovery room for about an hour and then sent to your room (inpatient) or sent home (outpatient).
“All surgery comes with some risks: risk of bleeding, infection and injury to something inside. You also have a 1 in 60,000 risk of dying from anesthesia, but you are much more likely to die driving your car, especially in the winter when there are a lot of idiot drivers around.” (For the curious among you, the risk of death from a motor vehicle accident is 1 in 103. I can’t find the odds of dying from stupidity, but the Darwin Award people keep a nice tally.)
If I was tying a woman’s tubes (tubal ligation), I added this:
“You also need to understand nothing is perfect, including tubal ligations. About three out of every 1000 women getting their tubes tied get pregnant, sometimes many years later. A few of those pregnancies will end up in the uterus, but many get stuck in the tube, causing an ectopic pregnancy which can kill you if not treated. So, if you ever think you are pregnant, you need to see a physician right away.” (I met a woman in Tennessee who had an ectopic pregnancy 13 years after her tubal ligation. She had been bleeding vaginally (and internally) for a few days, not realizing she was pregnant. I found 1300cc of blood in her abdomen.)
Now, that approach was too vague and informal for Ms. “Expectation Management” who thought researching every possible surgical complication was a fine idea, and then expected ME to grill my surgeon on how the team was prepared to avoid them.
Compartment syndrome – excess pressure in leg muscle spaces from being in stirrups for a long time, muscle damage from which may necessitate amputation
Pelvic lymphocele – collections of fluid in the pelvic cavity from removing lymph nodes, or hydrocele – collection of fluid in the scrotum causing it to swell to the size of a cantaloupe
Atelectasis – collapsed lung tissue from not breathing deeply enough, leading to pneumonia or respiratory failure requiring ventilator support
Deep vein thromboembolism (DVT) – a clot in the deep leg veins which can potentially break off and travel through the heart and into the lungs, causing instant death from a saddle embolus
I know a lot of the possible complications, which is why I hated gyn surgery! I’m more like Peg’s sister, Michele: Ignorance is bliss.
The day before surgery I had to drink only clear liquids and do a bowel prep. I drank a bottle of magnesium citrate, which is far easier to take than the gallon of NuLYTELY® I had for my colonoscopy prep. But, because a bowel prep can screw up one’s electrolytes, they told me to drink a 20oz bottle of Gatorade four hours before surgery. Yep, 3:30 a.m. Sleep is overrated.
We arrived at the hospital parking lot about 5:30 a.m. and trekked what seemed like a couple of miles to Surgical Registration. I checked in with a woman who was too alert for such an abysmal time. We waited for about 20 minutes, then someone led us on another trek to Pre-Op where I changed into a hospital gown and hopped onto the gurney.
My nurse was an adorable, diminutive redhead with freckles and a pixie cut, too alert and too cheery. She put EKG leads on my chest, a blood pressure cuff on my arm, and poked my finger to check my blood sugar, and started an IV, all while telling me what I needed to do.
“You remind me of my wife.” “Hey, you brought her here, I didn’t.”
I started laughing so hard she had to retake my blood pressure after I calmed down.
I talked with Dr. Pierce, the anesthesiologist, and reminded him of my paradoxical reaction to Versed (midazolam), a drug used for anesthesia induction and conscious sedation. Dr. Fine appeared a little after 7:00 am for some last-minute discussion and reminders. Surgery would take about two or three hours and I would go home in the afternoon if everything went well. Then the OR nurse put a bonnet on me, had me kiss Peg and rolled me down to the room. I slid onto the table while the anesthesiologist and the scrub tech introduced themselves and got me ready. The last thing I remember hearing was, “This might sting a little as it goes into your vein.” Click here if you want to see Robotic Assisted Laparoscopic Radical Prostatectomy .
When I woke up 3½ hours later, it seemed as if only ten minutes had passed. I felt pretty good in large part to the local anesthetic injected around the trocar sites. Even the catheter wasn’t uncomfortable. I had something to drink and the recovery room nurse had me walk down the hall. I was home by 3:00 and really happy I didn’t have to stay in the hospital.
The following week wasn’t bad, either. I didn’t have to get up at night because of the catheter. Peg got up at 1 a.m. that first night to empty the bag, but I cut my liquid intake in the evening and emptied it about 11 p.m. which got me through the night. I had six stab wounds for the trocars but only one hurt if I coughed or move wrong, and that only lasted a week. I took three hydrocodone tablets, mostly at night, and used acetaminophen the rest of the time.
My incisions
The pathology report came back by the end of the week:
Surgical pathology report Prostatectomy Pathology Report. A. Right neurovascular bundle margin, excision: -Neurovascular tissue, negative for malignancy. B. Prostate, radical prostatectomy: -Prostatic adenocarcinoma, Gleason score 4+5 = 9. -The margins of excision are negative for tumor. -Focal extraprostatic extension, left posterolateral, for a total span of 5 mm. -Uninvolved seminal vesicles. C. Bilateral pelvic lymph nodes, excision: -Six lymph nodes, negative for tumor (0/6). D. Posterior bladder neck, excision: -Fibromuscular tissue, negative for tumor. E. Anterior bladder neck, excision: -Fibromuscular tissue and focal urothelium, negative for tumor.
So, the cancer cells were worse than the biopsy and it had already peeked out beyond the prostate. Having negative margins means the bad stuff was confined to what was taken out. Surgery turned out to be the more prudent approach.
The catheter came out the following Monday. I had to change underwear frequently for a few days but was back to my pre-surgical level of incontinence by the end of the week. It felt strange being able to urinate like I did before my prostate started squeezing my urethra.
I had an appointment for the Vacuum Erection Device Clinic in January, but that is a whole ‘nother story.
I went to Costco
today. They had the normal entrance blocked off and routed people through the
cart entrance. (T-W-Th 8-9am are old people hours). They had the walk along the
side of the building partitioned with pallets and carts. We had to walk down
the sidewalk, around the end and back to the entrance. We got our carts but had
to wait in line because they were limiting how many people could be in the
store. They had TVs playing a PSA loop featuring Drs. Fauci and Birx, and Dr.
Jerome Adams, the US Surgeon General, explaining why we have to keep six feet
(or one alligator) distance between us.
We got to go in
when some number of people exited. The meat counter was pretty much empty. No
ground beef, save for a few packages of “organic” stuff: 4lbs that was going for about $21. Two packages of
stew beef. High end beef going for $30/lb. Five six-packs of boneless chicken
breasts. No thighs, no whole chickens. There was plenty of salmon and tilapia as
fish doesn’t have the same processing plant issues (and likely because it’s too
healthy for some people).
They had plenty of
fresh Italian sausage in the pork section. I suspect they ground up what little
pork they had left to stretch it out. I also saw a lot of the Kirkland bratwurst
(which I think is better and bigger than Johnsonville’s brats). The freezer
section had a lot of prepackaged stuff like beer battered cod, pulled pork,
sirloin burgers and half a pound of blackened mahi-mahi for $20. Ouch.
Most people kept
their distance, pausing at aisle intersections like 4-way stops, but some
wandered aimlessly, oblivious to their surroundings and crowding the rest of
us. One poor older woman was asking if Costco was handing out masks; the
staffer said, “It’s OK for now; you don’t have to wear
a mask until May 1.”
One Costco staffer
directed people to the checkouts as they became available. The cashiers were
behind 2×6 ft acrylic barriers and everything seemed to go smoothly. But
everyone looked grim. As Walter
would say, “Get your shit and get out!”
We are fortunate there are only two of us. We aren’t waiting for an unemployment check that won’t come anytime soon because the unemployment website is overwhelmed, and no one can apply (or was deliberately sabotaged by a cruel governor). We don’t have a houseful of kids that we have to home school while also working at home and THEN have to worry about feeding after a long day. We’re not in unimaginably long lines at food banks.
We’re the richest country in the world and our government is wasting $8,000 and 1,200 gallons of fuel per hour per jet flying twelve F-16s over cities filled with people who can’t go out of their apartments. If they do, they’re ignoring social distancing, so why bother mandating something people can conveniently ignore? It’s more of a tribute to a feckless leader than to the people risking – or taking – their lives. Bread and circuses.
There is a lot of misinformation and bad advice circulating regarding the COVID-19 pandemic. I’ve tried to provide pertinent and useful information in this blog post. But before I begin, I want you to do two things:
DON’T PANIC DON’T BE STUPID
Panicking in a crisis does no one any earthly good and often
makes things worse. This is not the zombie apocalypse, Outbreak, The Stand, Contagion or The Walking Dead. It’s
not even The Hot Zone, a book
and miniseries based on the
discovery of an non-human primate Ebola virus in Reston, VA in 1989.
We can get through this by helping each other, not by being
a selfish asshole hoarding toilet paper, or going out to restaurants because Devin
Nunes told you to. Follow current recommendations and guidelines to
minimize the risk of getting it or giving it to someone who is at greater risk
of dying.
Now, back to our previously scheduled PSA
What is Coronavirus? Coronavirus is a family of RNA viruses – chunks of genetic material in a protein capsule – that infect human respiratory tracts. Coronavirus, like the more well-known rhinovirus, respiratory syncytial virus (RSV) and parainfluenza, often cause nothing more than a common cold. It is so named because there are spikes on the surface that make it look like a solar corona. Click here to see an electron micrograph.
Where did it come from? Coronaviruses are “zoonotic” – transferred from animals to humans. Bats provide a reservoir for coronaviruses and spread them to other animals. SARS was thought to come from civet cats in Guangdong, China, while MERS was transmitted by dromedary camels in the Arabian peninsula before spreading to other countries. (MERS resurfaced in Saudi Arabia in October 2019.) SARS-CoV-2 might have originated from an outdoor wet market in Wuhan, China. Neither the Chinese nor the United States developed it as a bioweapon.
How is it spread? Coronavirus, like other respiratory viruses, spreads among people through droplets from coughing or sneezing which are then inhaled. It can also spread when hands contaminated with virus touch eyes or nose, or someone else’s hands.
The incubation period (time from contact to developing
symptoms) is 5-7 days but can be as long as 14 days, the rationale for a 2-week
quarantine. People who carry the virus can spread it even though they feel
fine. Health officials estimated a lawyer
with COVID-19 in New Rochelle, NY, had contact with 50 people before
becoming ill.
No one is sure how long the virus survives on surfaces like
countertops, handrails and boxes, although study
results published in the New England Journal of Medicine on March 17, 2020
found coronavirus lasts longer on plastic and stainless steel than on copper and
cardboard. When in doubt, wear gloves and wipe it off!
If coronavirus is common, why should I worry? Viruses, like bacteria, can mutate into more deadly forms. The virus causing the current disease, COVID-19, is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Yes SARS (Severe Acute Respiratory Syndrome 2003) and MERS (Middle Eastern Respiratory Syndrome (2012) were both “novel human coronaviruses,” meaning they hadn’t been seen in humans. The difference between coronavirus causing a cold and SARS-CoV-2 is like the difference between the E. coli in your intestine and E. coli O157:H7. The former keeps your digestive tract healthy while the latter caused severe illnesses and deaths in people eating contaminated hamburger (1993), “organic” spinach (2006) and Romaine lettuce (2019).
Isn’t it just like getting influenza? There have been an estimated 34 million influenza infections in the United States over the six-month 2019-2020 season with 375,000 hospitalizations and 22,000 deaths. But we have a vaccine and herd immunity for influenza, so the death rate is about 0.06%. There is no vaccine for COVID-19 and there won’t be one for 18 months or more. COVID-19 is more likely to kill people over 60, those with chronic illnesses (diabetes, asthma/COPD, heart or chronic kidney disease), and anyone with compromised immune systems (cancer, HIV, genetic disorders), regardless of age. The youngest death was a 21-year-old Spanish soccer player with undiagnosed leukemia and coronavirus.
“…Between 160 million and 214 million people in the United States could be infected over the course of the epidemic, according to a projection that encompasses the range of the four scenarios. That could last months or even over a year, with infections concentrated in shorter periods, staggered across time in different communities, experts said. As many as 200,000 to 1.7 million people could die….”
Take a deep breath and don’t panic. England got through WWII
with “Keep Calm and Carry On,” not, “OMG, it’s the apocalypse and I’m going to
run out of toilet paper!”
Wash your hands, often! Wash them for 20 seconds, the time it takes to sing “Happy Birthday” twice or recite the Star Trek intro. Hot water isn’t more effective than cold or warm water, so don’t scald yourself.
Use hand sanitizer if you’re out and don’t have soap. Antibacterial wipes are good for public surfaces (shopping carts, handrails).
Don’t touch your face. That is going to be really hard for most people. Cajun hand sanitizer will make you remember not to touch your face!
Although it’s better than using your hand, I don’t think coughing or sneezing into your elbow is a great idea. Get a small pack of tissues or stuff some in a zip-lock bag and keep them handy when out. Use them and toss them in the trash. And use hand sanitizer afterwards.
Stay away from crowded places like subways, commuter trains and airplanes unless absolutely necessary. Many businesses are making their employees work from home.
If you need catchy music to grab your attention, then watch
this Vietnamese PSA.
Should I wear a mask? In general, no. Regular surgical masks stop droplets, which is helpful but won’t filter out viruses. If you are healthy and out in public, you don’t need one. N 95 respirators, masks that can block 95% of particles down to 0.3 microns, are used by people exposed to dust and other small particles. Health care N-95 respirators are a subset, specifically for health care workers. They need to be fitted to be effective and are a bitch to breathe through.
You should wear a mask if:
You are a health care worker.
You are coughing or sneezing.
You are sick and need to leave the house
You are sick and can’t isolate yourself from healthy housemates
Why should we practice “social distancing?” Because health officials want to avoid an exponential increase in coronavirus cases by “flattening the curve.” (If you don’t understand exponents, you weren’t paying attention in algebra class and I don’t have time to explain them! Just think “increasing really fast.”) We don’t want a lot of people getting sick in a short period of time and overwhelming the health care system. It is better to spread out those illnesses over many weeks or months.
Protecting the vulnerable – those who are elderly or have
compromised immune systems – is the single best reason for keeping your
distance from other people.
How is COVID-19 treated? Like any other viral illness there is NO cure. One treats the symptoms whether cough, fever or full-blown respiratory failure requiring mechanical ventilation. Influenza is often treated with oseltamivir, which shortens recovery by 1 to 2 days. Remdesivir, created from a molecule developed ten years ago, may be the best drug to treat COVID-19, but it’s only in the testing stage and it isn’t a cure.
Eating garlic, drinking bleach or colloidal silver,
breathing hot air from your hair dryer, taking Vitamin C or zinc, snorting
cocaine or masturbating
will not protect you from COVID-19.
What should I do if I feel sick? If you just feel crappy with mild to moderate viral symptoms – cough, fever, aching – call your healthcare provider. DO NOT go to the Emergency Room without being told to! They don’t want to see your sorry ass for something that is not life-threatening and will just have to run its course.
However, if you are having chest pain or enough difficulty
breathing that your lips are turning blue, or you feel as if you are drowning, GO
TO THE EMERGENCY ROOM IMMEDIATELY!
Should I be tested? Not unless a qualified healthcare worker thinks you need to be tested.
There aren’t enough tests right now.