What I started writing at 2am the night after my knee surgery
There are many unforgettable scents I’ve come across throughout life that I can imagine just by my memories. How many do you recognize?
Babies and puppies have their own warm, comforting scent, like that new car smell without the chemical outgassing.
The Sonoran desert in Arizona is home to a variety of hardy aromatic plants: desert willow; creosote bush; mesquite trees. I still remember what Sabino Canyon, northwest of Tucson, smells like in the searing midday heat.
Sonoran Desert landscape, Arizona
I found a decaying animal carcass along the Route 80 bypass just above Spring Canyon Road in Bisbee, Arizona when I was eight. There wasn’t much left, just a ribcage and desiccated but still rotting flesh, but the acrid smell was unforgettable.
I sometimes roamed the drainage ditch that ran along Tombstone Canyon in Bisbee. I would build earth dams across areas of flowing water, creating a reservoir I’d then destroy with imaginary Allied bombers (usually a stick). I remember the smell of wild mint among the sparse fauna. Now I would be afraid of contracting some water-borne illness like Naegleria, the brain-eating amoeba.
Eddie Rojo’s tavern in Bisbee had a shuffleboard table I’d play with while my stepfather indulged in his favorite pastime, soaking his regrets in Falstaff. The table had fine sawdust in the gutters which competed with the smell of old beer in the tavern’s floorboards. I liked sliding the heavy pucks up and down the butcher block playing surface that was smooth as glass.
I used to have an olfactory hallucination at night when I was little, which I can only describe it as “spoiled mustard.” I’ve never run across that smell when awake.
My grade school in Arizona had an auditorium that doubled as the lunch room. Kids’ sack lunches sat there unrefrigerated until noon. The pungent, nauseating odor coming from the contents usually made me puke on the table. The lukewarm milk cartons also had their own unsettling smell.
Mrs. Frost, my first-grade teacher, wore a very distinct perfume which I found very comforting. Thirty years later I instantly recognized that scent when my medical assistant Eileen wore it one day. She told me it was White Shoulders, created during the 1940s and still popular.
There was nothing like the smell of ditto ink coming from a warm test paper, fresh off the printer. We hold them against our faces and inhale before starting the exam. Generations of schoolchildren will never experience it.
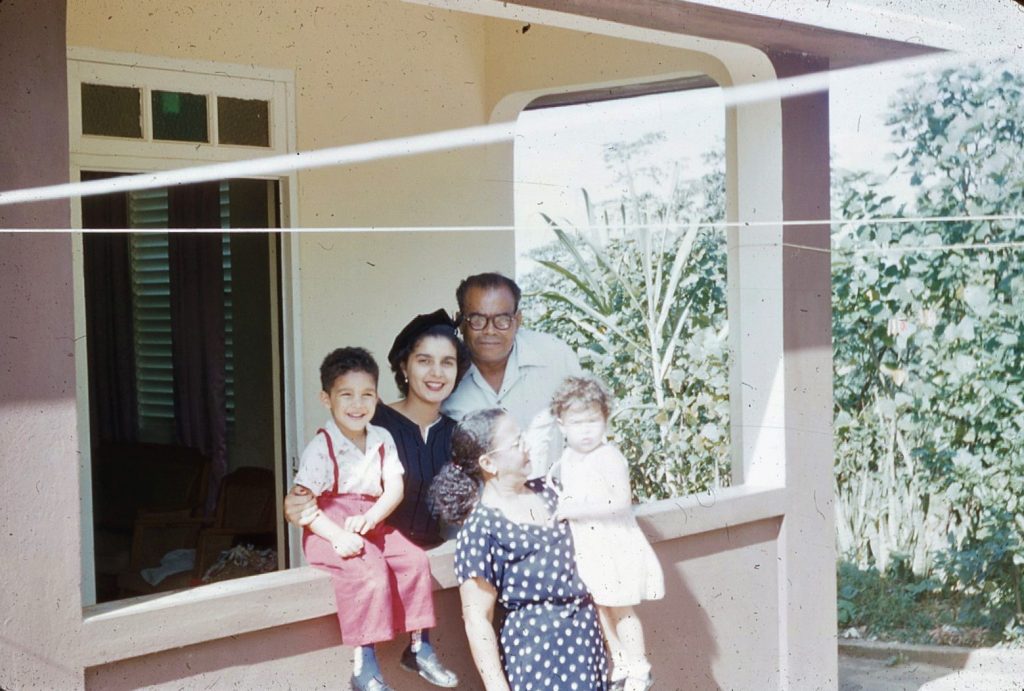
I don’t remember my grandparents’ concrete house in Puerto Rico having window screens. At night our beds were enveloped in tents of mosquito netting laced with pyrethrum, an insect repellent derived from chrysanthemums. I can still smell it.
Family in Vega Baja, PR 1957
One didn’t need a clothes dryer in the desert, even in the winter. One of life’s greatest pleasures is taking in the fresh scent of bedsheets or clothes after they’ve dried outside, something no laundry product can match.
Winter in Bisbee, AZ, 1960
We were friends with a couple that had seven children, five of which were crammed into several beds in a small room. The mattresses were old and likely peed on several times over the years. I remember being 8 years old sleeping on one of those mattresses with one of their girls while our parents played cards into the night.
Back during the 1950s and 1960s most doctors’ offices had a strong antiseptic smell, most likely from isopropyl alcohol. It always made me think of those long, reusable hypodermic needles soaking in those stainless steel trays and the big glass jars of cotton balls and tongue depressors.
The scent of blooming flowers in the spring – roses, lilacs, apple and cherry blossoms – represent new life after a soul-killing winter.
Lilac Blossoms
That comforting, clean air smell after a fresh rain is called petrichor. Some it comes from lightning splitting atmospheric nitrogen and oxygen, which recombine into ozone and nitric oxide. Another component is geosmin, produced by Actinomycetes, a bacteria found in soil.
Mount Washington, NH
Most people in temperate areas look forward to burning dead leaves in the fall. Those of us with chronic lung disease dread the smoke and many municipalities have outlawed open burning. Burning the evil weed, along with the red eyes, giggling and munchies, is a different story.
Autumn leaves in Gorham, NH
Wood-fire smoke comes in several varieties:
the hot, dry wood smell of a sauna
cozy when sitting around a fireplace in winter or a fire pit in the summer
oddly unsettling when it permeates everything in a house that has been heated solely by firewood
terrifying when it comes from the raging forest fire beyond the horizon
The air at sub-zero temperatures has a crisp smell largely because there are so few odiferous molecules in the air.
Svalbard Island, Norway
Everyone remembers having the pine scent of a fresh Christmas tree filling the house. I stopped getting real trees thirty years ago because the pesticides and preservatives caused bronchospasm. I take solace in the bags of cinnamon-scented pine cones that Jewel sells every year.
Christmas 1962
The dead mouse in the wall behind our range had an unmistakable musty odor. My two “helpers,” a cranky Lhasa-Apso and a greyhound with “a great nose,” tasked with helping me locate the carcass, sat in the family room and laughed while I drilled three holes between the studs before finding it.
The pseudomembrane of the upper respiratory tract produced by diphtheria infection is said to smell like a wet mouse, though I’ve never encountered either.
I reached a milestone in 7th grade when I realized that foul body odor was coming frtom my own armpits and it was time to start using deodorant.
The eye-watering rotten-egg smell of hydrogen sulfide, is “rancid” when in reference to a particularly noxious fart, but “smells like money” if you own a petrochemical refinery.
I stopped at a turnout on a back country two-lane and sat at the lone concrete picnic table under the trees. I noticed a slightly sweet but pungent odor nearby; it came from a cool, dusky pile of human feces about ten feet away. Someone must have been really desperate to drop a deuce on the side of the road. Well, when you gotta go…
There is absolutely nothing like the intoxicating, primal scent of an aroused woman’s vaginal secretions, now indelicately known as “wet-ass pussy.” I’ll never forget my first encounter, forbidden yet exciting! Regrettably, women lose that aspect of arousal with age.
Abstract vulva in fabric
Not everyone likes it; many young men who lack both discriminating olfactory epithelium and finesse find it “disgusting.” The “personal hygiene” industry preys on women’s insecurities to sell crap, promising they’ll smell “fresh as a daisy.”
Fresh semen has its own unique odor, though I doubt most women find it alluring.
Human blood has a slightly metallic odor, especially when encountered in large quantities, such as after a postpartum hemorrhage, or on the floor around the operating table on which the dead guy with a .22 hole through his heart lay.
Para-dichlorobenzene gives mothballs and urinal cakes their pungent smell, which I’ve also detected in a couple of really poorly-maintained home bathrooms.
The black knobs on the lids of some cooking pots are made of phenolic resin, made from combining phenol and formaldehyde. They emit a very unpleasant odor after being heated in an oven.
It’s been said everyone has opinions and they all stink. Also that politicians and dirty diapers need to be changed frequently for the same reason.
“Inside every old person is a young person wondering what the hell happened.” Unknown but perceptive
My 50th high school class reunion is this year. The prospect is at once fascinating (I never thought I’d live this long) and terrifying (some memories never die). But I started to think about those who attended their 50th reunion in 1972. We had our whole lives ahead of us while they were headed into the twilight. Now it’s our turn to ride into the sunset.
The First Fifty Years
The class of 1922 lived through two world wars, the 1918 Spanish flu pandemic and the Great Depression. They were the Greatest Generation, lauded for their patriotism, sacrifice and service, and the grandparents of my generation, the oft-maligned Baby Boomers. During their half-century, they witnessed profound changes in technology, life and culture.
Automobiles went from the Model-T through the gangster cars of the 1930s, the two-ton hulking sedans of the 1940s, the T-Bird and the ’55 Caddy with enormous fins, the Corvette, the early ‘60s Lincoln Continental convertible with suicide doors, the Ford Mustang, to the 1969 Chevy Camaro Bumblebee.
The Wright Brothers’ first airplane became the open-cockpit biplane, the twin-engine propeller driven Douglas DC-3, the Boeing 707 with four jet engines, and then the Boeing 747, which debuted in 1969.
Only sixty-six years separated the flight at Kitty Hawk and the first moon landing.
Musical genres exploded over those 50 years: gagtime, big-band, country and western, swing, jazz, easy-listening, early rock-and-roll, R&B, and what we call “classic rock.” Duke Ellington. Benny Goodman. Count Basie. Sinatra. Elvis. Buddy Holly. The Beatles and the Rolling Stones. Woodstock was in 1969, three years before their 50th, but they were horrified by those “goddam hippies with their free love and drugs!”
Recorded music started out as wax cylinders played on a wind-up gramophone in the late 1800s. Emile Berliner created the first flat disc recording in 1892. The heavy and brittle shellac 78 rpm records in monaural became popular in 1925. By the 1950s 33⅓ rpm vinyl stereo records replaced “78s.” 45 rpm discs offered cheap singles. Reel-to-reel tapes were reduced in size to the cassette and the 8-track. The in-dash cassette player debuted in 1968
Telephones, popular since the early 20th century, became smaller and available in colors other than black. Dials were replaced by push button “touch-tone.” Bell Systems introduced the Picturephone at the 1964 World’s Fair in New York, but it cost $160/month to lease one of these puppies.
The heavy floor-model radios of the 1920s became smaller and portable over the next 40 years. Transistors replaced vacuum tubes, making radios portable, like the cheap Japanese pocket models with the terrible earpiece we remember from high school.
Television, which started as a toy for the rich in the 1920s and 1930s, became more popular and affordable during the 1940s. Screens became bigger during the 1950s and we could get color televisions by the mid-1960s. People with a lot of disposable income could buy an all-in-one console with a television, AM/FM radio, and a record player. Try stealing THAT from someone’s house!
ENIAC, the first electronic programmable computer, was introduced in 1945. It weighed 27 tons, took up 1,800 square feet and needed 150 kW of electricity to operate. The “slightly smaller” UNIVAC computer (only 14.5 tons) debuted in 1951, followed by IBM’s mainframe computers into the 1960s.
Smallpox and polio vaccines prevented devastating illnesses. Our mothers lined us all up for the smallpox inoculation that left dime-sized scars on our left arms. We got our oral polio vaccines in sugar cubes. Fluoridated water, the bane of conspiracy theorists, helped prevent tooth decay in people, regardless of socioeconomic status. Government inspections of our food supply have greatly diminished, but not entirely eliminated, food-borne illnesses. Infant and maternal mortalities have dropped precipitously!
What a time to be alive! But all mythically wonderful eras have dark sides.
The people who made it to 1972 were lucky. The life expectancy for those born in 1904 was 47 years, and only if you were white. Infant mortality was 157 per 1,000 live births. Many died from infectious diseases in the pre-antibiotic era. The common folk often worked in grueling physical jobs which left them worn out by their late 50s or early 60s. Men commonly dropped dead from “the big one” in their mid-sixties.
Racism was rampant and largely accepted. D. W. Griffith’s movie Birth of a Nation spurred the revival of the Ku Klux Klan during the 1920s and lynching was common. George Wallace promised “Segregation today, segregation tomorrow, segregation forever!”‘ It took the Voting Rights Act of 1965 to force Southern States to comply with the 15th Amendment, ratified 95 years previously.
Society expected little of women other than to stay at home, raise children and obey their husbands. Few women worked outside the home until WWII, when they were called into factories to replace the men sent overseas. When the war ended they were expected to return to their traditional roles so the menfolk could “provide for their families.”
Still, we remember the good more than the bad and the ugly.
THE SECOND FIFTY YEARS My classmates are part of the Baby Boomers, maligned by Gen Xers and Millennials (with some justification). We’ve probably seen the extensions and improvements of prior advances more than truly phenomenal innovations but neither should be dismissed as irrelevant.
Those classic cars of yore were also death traps. Accident reports of people flying through windshields or being crushed by engine blocks, children being decapitated by metal glove box doors, and occupants being incinerated by ruptured gas tanks were common. Ralph Nader’s damning book, Unsafe at Any Speed: The Designed-In Dangers of the American Automobile, criticized the auto industry’s resistance to safety concerns and led to the creation of the National Highway Traffic Safety Administration in 1970. Research and engineering resulted in mandatory seat belts, crumple zones, safety cages and airbags minimizing passenger injury. More recently, manufacturers have introduced lane departure warnings, collision avoidance systems, automatic braking and stability control.
Air travel, once only available to the well-heeled, is now accessible to everyone. Aircraft safety has improved greatly since the 1950s so that you’re more likely to die from riding a bicycle, driving a car, or being struck by lightning.
While we haven’t returned to the moon (yet), we’ve witnessed the development of the space shuttle, the International Space Station and the Hubble and James Webb telescopes. NASA developed technologies we take for granted: Lasik, functional artificial limbs, the insulin pump, wireless headsets and the Dust Buster. But we also have a billionaire giving rich people with more money than sense carnival rides into “space” on top of a dick rocket.
I still think Classic Rock is among the best, but I switched to jazz as I’ve aged. Disco was amusing. There was some good music during the 1980s and maybe the 1990s, but, at least to me, the only things rap needs are a rhyming dictionary and uncontrolled anger. Most of us remember that fateful day when we became our parents, asking our kids, “What is that shit you’re listening to?” Maybe rap is the 21st century version of 60’s protest songs.
Digital storage media – the compact disc and digital video – replaced vinyl records, cassettes and videotape. Apple Inc. went further and gave us even more compact storage and playback with the various iterations of the iPod. My 160G iPod classic currently has 16051 songs loaded, enough music for more than 50 days. (Oddly enough, a younger generation has resurrected vinyl records for some obscure reason. We switched to CDs because vinyl gets scratched and your record eventually sounds like frying bacon!)
The evolution of the telephone is both a marvel of engineering and a scourge. We grew up with party lines and wired telephones (which we RENTED!). Captain Kirk’s fictional communicator became the first flip phone, was rendered obsolete by smart phones and has now returned as the foldable phone, running anywhere from $400 to $1500. Now Millennials and Gen Zers use their smart phones to do everything, except make phone calls.
The last telephone booth in New York City was taken out on May 23, 2022. I guess Clark Kent will now have to change into his Superman outfit in the bathroom of one of the 241 Starbucks. Dick Tracy’s wrist radio, once the stuff of science fiction, is now the smart watch, giving younger people another way to ignore phone calls.
Does anyone have a portable radio anymore? Does it matter? I can stream broadcasts from anywhere in the world, from Iceland to New Zealand.
Televisions have gotten bigger, lighter and with much better resolution. The “wall television” from Ray Bradbury’s Fahrenheit 451, complete with interactive capabilities, has taken over some households. We had three network channels in 1972 and maybe a couple of local stations if you lived near a large city. Now cable is ubiquitous, rapacious, aggravating. Five hundred channels and nothing to watch.
Tired of cable companies and commercials? Cellular companies are offering internet services and digital antennas provide HD programming without rabbit ears or those bulky outside aluminum UHF/VHF aerial antennas of old. Streaming services have changed viewing habits, opening up international programming to new audiences.
The guidance computer used by the Apollo 11 team had 64Kb of memory and a 0.043MHz clock speed. My first PC, which I bought in 1990 for about $3000, had a 286 processor with a blazing clock speed of 16MHz, 1MB RAM, a 30MB hard drive and ran on Windows 3.1 My 2017 Samsung Galaxy S8 has 64GB storage, 4GB RAM, four cores at 1.9 GHz and four cores at 2.35 GHz, a 1.9GHz clock speed, a 12 megapixel camera, Bluetooth connectivity and Wi-Fi capability. So my phone has 64 million times more memory, is almost 45,000 faster and can perform hundreds of millions more instructions than the Apollo computer. Advanced technology so one can watch cat videos while sitting on the toilet.
We’ve been through an epidemic and a pandemic. HIV/AIDS appeared visibly in 1981, although the earliest known case of HIV infection was identified in a man who died in Kinshasa, Congo, in 1959. Back then HIV infection was a death sentence; then we discovered some infected people survived. Now we have drugs that make HIV virus levels undetectable.
The SARS COV-2 (coronavirus) pandemic started in late 2018. As of October 1, 2022, coronavirus has infected more than 623 million people and killed 6.5 million. Three COVID vaccines – Pfizer, Moderna and Johnson & Johnson – were developed in less than a year, a feat that in the past has taken years if not decades. (And no, 5G does not make your body more susceptible to coronavirus infection and Bill Gates isn’t trying to microchip your body with the vaccine. That smartphone in your hand and social media already track everything you do, but you’d rather die than give them up, right?)
The next fifty years Assuming humanity has pulled its collective head out of its ass and not destroyed itself in a nuclear Holocaust or from making the planet uninhabitable, the Class of 2022 will have lived through their own set of wondrous advances by 2072. While visions of the future often miss wildly, I’d like to offer my own predictions.
Self-driving cars won’t run into pedestrians or other vehicles, and will be powered by something other than fossil fuels.
Most, if not all, towns and cities will be eco-friendly, running on solar power, like Babcock Ranch in Florida, which weathered Hurricane Ian with no disruptions.
Cancers therapies will include genetic manipulation, nanoparticles and biologics with little or no adverse effects on the patient. People will wonder why we used barbaric treatments like radiation, chemotherapy and major surgeries.
Society will be better prepared for pandemics and there will be minimal whining about public health mandates focused on “the greater good.”
No one will understand why we tolerated homelessness for so long.
Cubs fans will still have to wait another 44 years for a World Series victory.
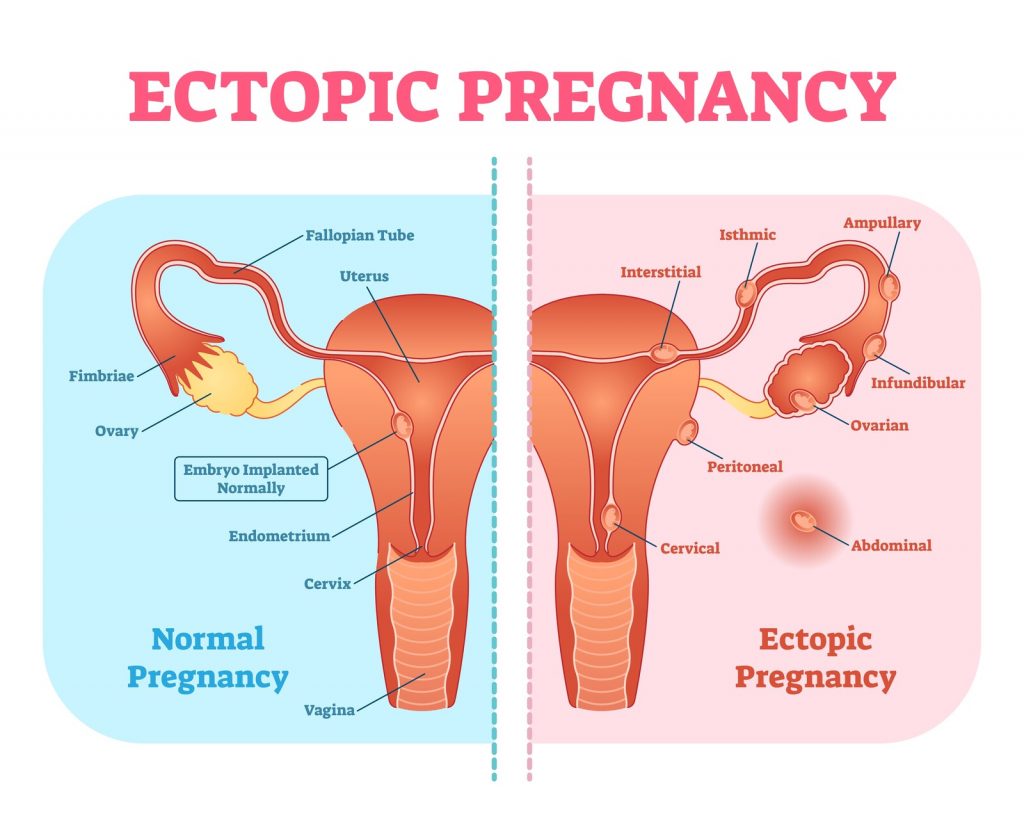
A pregnancy starts when a Fallopian tube sweeps up an egg like a shop vac and sends it down towards an army of sperm lying in wait. While it takes one sperm to fertilize an egg, it takes hundreds of them to break down the zona pellucida, the egg’s barrier to fertilization.
When that happens, the lucky bastard yells, “I’ve got you now, my pretty,” and thrusts himself into her. Now joined in holy matrimony, the fertilized egg – a zygote – takes a short honeymoon trek down the tube, developing into a blastocyst on its way the uterus. There it implants, sets up housekeeping and watches Netflix for the next nine months.
But that doesn’t always work that way. The blastocyst may attach itself somewhere outside the uterus in an “ectopic” location that wasn’t designed to grow a full-term baby. Those sites include the Fallopian tube (the most common); the cornua (where the tube attaches to the uterus); the cervix; an ovary or inside the abdomen.
An ectopically implanted pregnancy is more likely in a woman whose tubes have been damaged by infection, endometriosis, or previous abdominal surgery, including tubal ligation. Using an IUD for contraception increases a woman’s risk. Even a woman who has had a hysterectomy but with an intact ovary can become pregnant, likely earning her a place in the tabloids.
An abnormally implanted pregnancy can only grow so much before the tissue around the implantation site blows apart and all hell breaks loose. Internal bleeding can be massive and a woman will die from hemorrhagic shock if not treated promptly.
The Arab Spanish physician Abulcasis (Arabic name: Abul Qasim Khalaf ibn al-Abbas al-Zahrawi al-Ansari), was an impressive and accomplished dude who wrote Al Tasrif, a thirty volume medical encyclopedia, earning him a place among the “fathers of surgery.” He made the first known reference to ectopic pregnancy in the 10th century. Other physicians reported ectopic pregnancies during the next 900 years, largely discovered at autopsy as it was invariable fatal.
But by the mid 1800’s doctors were becoming more aware of the signs and symptoms of ectopic pregnancy. Timely surgical intervention saved the lives of many women but definitively differentiating an ectopic pregnancy from other conditions – an ovarian cyst, endometriosis, or appendicitis – remained problematic for the next 100+ years.
Such was the state of diagnostic abilities when I started my residency in 1979. A woman who came to the Emergency Room in obvious hemorrhagic shock – high pulse and low blood pressure – went straight to surgery. But if she presented with lower abdominal pain, a positive pregnancy test and sometimes brown vaginal bleeding – and was hemodynamically stable – we tried our best to confirm an ectopic pregnancy. The probability increased if, on pelvic examination, one felt a painful mass on either side of a normal-sized uterus, but there was still a 20% chance it was something else.
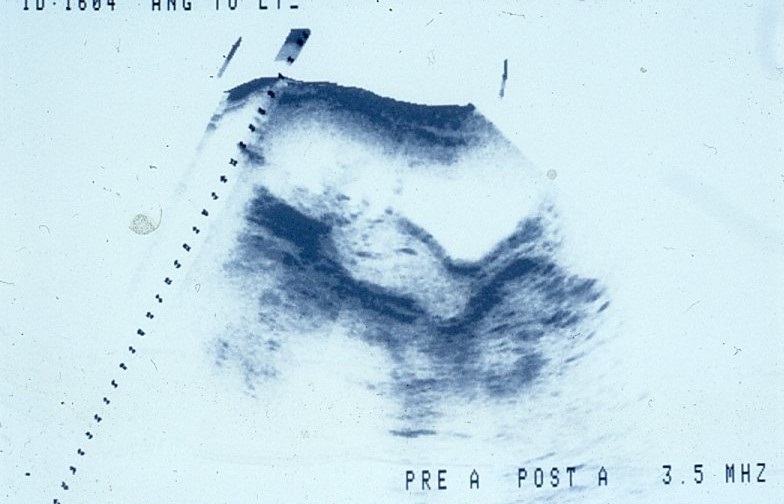
Ultrasound had been used clinically since the mid-1950s, but images weren’t great, appearing more like abstract paintings than pelvic organs. Radiologists’ interpretations were often ambiguous and usually unreliable when proclaimed with absolute certainty. One of my attending physicians opened up a woman’s abdomen after the radiologist said, “There is definitely an ectopic pregnancy here,” only to find absolutely nothing.
If we were still unsure and the woman agreed to it, we’d try doing a culdocentesis. That involved sticking an 18-gauge needle through the back of the vagina below the cervix, then pulling back on the plunger of a large syringe. (Yes, it’s as painful as it sounds, even after injecting local anesthetic into the area.) Sometimes we were lucky. If the syringe filled with “non-clotting” blood (blood that had already clotted and then broken down), we knew she was bleeding internally and likely had a ruptured ectopic pregnancy. If culdocentesis wasn’t successful and we still weren’t sure, we took the woman to the operating room for diagnostic laparoscopy sparing the woman an abdominal incision if everything looked clean.
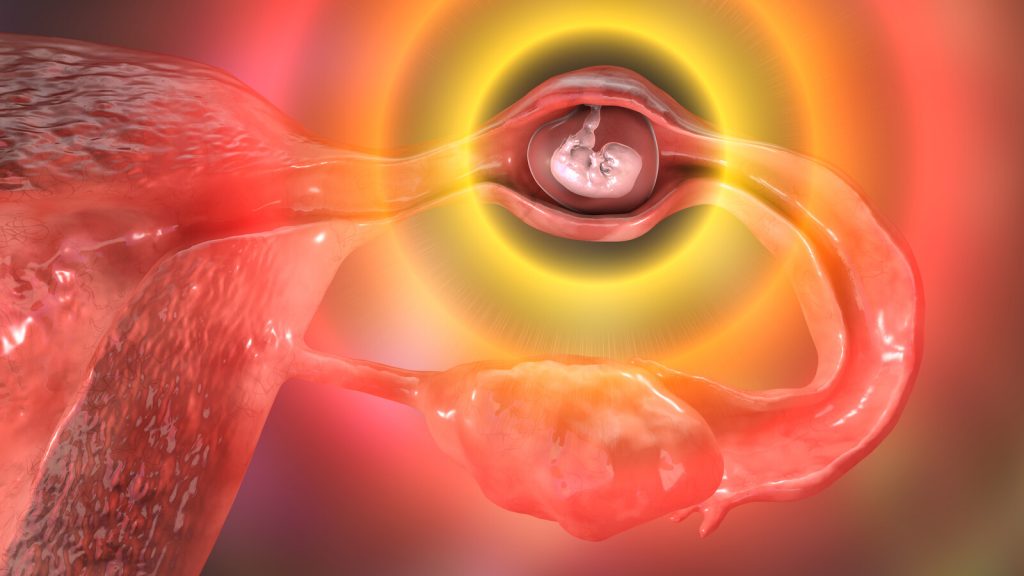
Tubal pregnancies are usually dark purple blobs, ranging in size from a pomegranate seed to a breakfast sausage, which may be leaking a little blood or actively hemorrhaging. There’s usually a small piece of placental tissue among the clot in the tube, but nothing that remotely resembles a fetus. I witnessed one notable exception during my residency. A tiny, live fetus, about the size of a grain of rice, was moving in the small gestational sac that had been expelled from the end of the tube. And no, there was – and still – no way to implant it into the uterus! Placental tissue, once disrupted, won’t reattach itself in the uterus.
We had three surgical options:
Opening the tube over the affected area, emptying out the contents and delicately sewing the incision shut, making sure there was no bleeding. The tissue was fragile and it was like sewing two sticks of room temperature butter together.
Taking out the damaged section of tube, leaving the ends for a skilled microsurgeon to put back together later on.
Taking out the entire tube because a badly-damaged tube made another ectopic pregnancy more likely.
A lot has changed since I started residency more than forty years ago.
Diagnostic testing
Simple urine or blood pregnancy tests, first developed in 1976 and referred to as “qualitative”, look for the presence or absence of human chorionic gonadotropin (hCG) a hormone produced by placental tissue. A positive test indicates a pregnancy somewhere in a woman’s body. A negative test usually means there is no pregnancy but the test will be “falsely negative” if hormone levels are too low to detect.
Structurally, hCG is made up of two pieces: the alpha subunit (α-hCG) which is also common to ovarian and thyroid hormones, and the unique beta subunit (β-hCG). Starting in the early 1980s, laboratories were able to assay blood for small amounts of this beta unit, the “quantitative β-hCG test.” We used the changes in hormone level over several days to monitor very early pregnancy development, hoping to distinguish normal pregnancies (single and multiple) from abnormal ones (blighted ovum, miscarriage, ectopic, the varied forms of molar pregnancy, or placental fragments leftover in the uterus after a miscarriage).
Measured in milli-International Units per milliliter (mIU/mL), hCG becomes detectable around the third week after a missed menstrual period. hCG levels should double every 48 hours in a normal pregnancy and transvaginal ultrasound should be able detect a gestational sac in the uterus at around 1,500-2,000 mIU/mL. One can reliably rule out an ectopic pregnancy after detecting a fetal pole (the earliest evidence of a developing embryo) with a heartbeat. (Simultaneous intrauterine and ectopic pregnancies occur spontaneously in less than 1:30,000 naturally occurring pregnancies, but that incidence increases to 1:100 to 1:500 with in vitro fertilization.)
hCG levels that rise more slowly, plateau or decline usually indicate an abnormal pregnancy. Combined with serial ultrasound examinations will lead to diagnosing:
A blighted ovum if there is an empty gestational sac with no fetal pole;
An inevitable miscarriage if there is a fetal pole larger than 7mm with no heartbeat
A miscarriage or ectopic pregnancy if there is only placental tissue in the uterus at levels where we would expect to see a gestational sac.
If physicians can’t rule out an ectopic pregnancy, they’ll scrape tissue out of the uterus (a D&C) and ask the hospital pathology department to look at the tissue while still in the operating room. If there’s only endometrial tissue and no chorionic villi, the vascular bridge between the uterus and placenta, there’s an ectopic lurking somewhere.
Imaging
Ultrasound image resolution has progressed from vague static images like this:
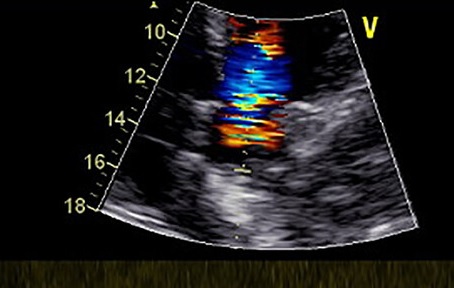
to detailed, real-time images such as this fetus (the four lines in the black area is the umbilical cord).
Color flow Doppler ultrasound can show blood moving in and out of an ectopic pregnancy in the adnexa, the area next to the uterus, which is helpful if the sonographer can’t distinguish a definite mass. (This, however, is Doppler flow of a heart, the only royalty-free image I could find.)
So, when a radiologist tells me, “There’s a 2cm mass with blood flow in the right adnexa, nothing but endometrial tissue in the uterus and a lot of echogenic material in the cul-de-sac running up the para-colic gutter,” I know I can skip the laparoscopy and open her up.
Surgical treatment
However, surgical treatment has also changed. Tubal ligation was the only surgical procedure we did in the early 1980s. By the early 1990s, physicians with far more balls than me, along with surgical instrument innovations, were starting to take things out of people laparoscopically. Removing an inflamed appendix became a simple outpatient procedure. Taking out a gallbladder full of stones using a laparoscope was far easier and less traumatic than the old days which required an incision along the right rib cage from stem to stern, and digging deep while your poor intern (me) tried to retract a six-inch deep wall of fat with a “Weinberg Vagotomy Retractor,” otherwise known as Joe’s Hoe (and it is as big as the garden tool).
“Pull harder, dammit!” “I’m pulling as hard as I can!”
Operative laparoscopic surgery had a steep learning curve in the early days and I was skeptical of the newfangled approach to ectopic pregnancy. I was suckered into assisting two youngsters with far more confidence than ability and both endeavors lasted two hours. One insisted in putting a trocar (which looks like a tent stake) through the abdomen in the vicinity of the inferior epigastric artery, despite my pleas to reconsider. She wasn’t concerned with the pulsating stream of blood and continued prospecting for the ectopic pregnancy.
I got a call one Saturday at midnight from the ER doc at a small hospital in Nebraska, 70 miles away from where I was working.
“I have a woman here with a ruptured ectopic pregnancy and I want to transfer her.” “You don’t have anyone there who can deal with it?” “Well, the general surgeon comes here on Wednesdays but I don’t think she’ll hold out until then. I’ve started a unit of blood and the ambulance is here.”
I was working as a locum tenens in someone else’s practice. I called the senior partner since he was rather protective of the practice’s reputation and I didn’t want to step on any toes. He wasn’t happy but met me in the Emergency Room. The woman arrived about 1:30am and, after introductions, examination and discussion, we were in the operating room at about 2:00am.
Setting up for an operative laparoscopy takes at least half an hour or more after the patient goes to sleep. The equipment includes:
a video camera and two monitors
the laparoscope light source
the CO2 insufflator used to blow up the abdomen like a balloon so the surgeon has room to work
an electrocautery unit
reusable instruments like the laparoscope and the insufflation needle
an array of expensive, disposable stuff like operating ports, instruments to cauterize vascular pedicles, a combination irrigation/suction device hooked up to room suction and a bag of saline,
and a uterine manipulator, which requires putting the woman in stirrups, putting on the surgical drapes, using a speculum to find and dilate the cervix before inserting it into the uterine cavity.
Laparoscopic surgery starts with putting in the insufflating needle just inside the belly button, the thinnest part of the abdominal wall, then filling the abdomen with enough CO2 so there’s room enough to work. After that, the surgeon inserts at least three or four ports in the abdomen: a 10mm for the laparoscope; a 5mm just above the pubic bone for a wand to move the innards around; and 5mm or 7.5mm ports on either side for operating instruments and grasping. (I have six abdominal scars from my robotic prostatectomy.) Click here for a great overview of laparoscopic trocar placement.
Older ports consisted of a stainless steel trocar with a pyramidal end like a tent stake inside a stainless steel sleeve which one pushed this through small incisions, taking care not to puncture the bowel, the bladder or the aorta. Newer ports are disposable plastic with more blunt trocars to minimize the chance of damage, but they take a little longer to work through the abdominal wall.
So, after setting up, gently and deliberately excising the damaged portion of tube, sucking out blood and clot, irrigating the pelvis, inspecting to make sure everything is clean and hemostatic, taking all the instruments out and closing the incisions, we were done about 90 minutes later.
My approach to an ectopic pregnancy in the good old days was direct. I’d make a small abdominal incision, grab the tube with a Babcock clamp, remove the offending ectopic, clean out the blood and clots in the pelvis, inspect the other tube and ovary, and then close her up in 20-30 minutes.
It’s one of many reasons I’m happy to pass the baton to a younger generation.
Medical Treatment
Methotrexate, a drug initially used to treat cancer and then rheumatoid arthritis, is sometimes used to treat unruptured ectopic pregnancy. There are stringent criteria for its use – a stable and reliable patient, a mass less than 3.5cm, hCG < 5,000 mIU/ml, and no detectable cardiac activity – and the woman must be monitored closely with serial hCG levels. Success rates are reported to be around 90% when used appropriately.
The emergency room physician at a small hospital in Tennessee called me around 11:30 pm on a Sunday night. A 42-year-old woman came in complaining of vaginal bleeding for a week and severe pain in her right lower abdomen. “She has a positive pregnancy test; her hemoglobin is 8 and her pulse is about 110.” A normal hemoglobin level for a non-pregnant woman is 12-16 gm/dl; even in pregnancy the level should be 11 or so.
I walked into the examination room and met a slightly pale woman on a gurney; her husband stood next to her.
“Hi I’m Dr. Rivera. I assume the ER doc has told you why I’m here?” “Yes, he told me I’m going to need surgery.” “Well, that’s a good place to start. Tell me what’s been going on.” “I started bleeding off and on last Monday. I didn’t think much of it, but it hasn’t stopped, and I started having pain in my side tonight, so I came here.” “Have you felt any pain in your shoulders?” “Yes, my right shoulder started hurting two days ago.” She noticed the look on my face and asked, “That’s not good, is it?” “Not really. If you’ve had internal bleeding the blood can irritate your diaphragm and your body interprets that as shoulder pain.” “Yes, but how can I be pregnant? I had my tubes tied thirteen years ago!” “Well, tubal ligations have an inherent failure rate. I saw one woman who got pregnant after her tubal. I took out her tubes after delivery and found an inch gap in both tubes.” “Really!”
So I took her to the operating room. My scrub tech was the Czechoslovakian grandmother who always made sure I was well-fed when I made rounds in the morning. I was sure I didn’t need to start with a diagnostic laparoscopy and went straight to an abdominal incision. She had 1300cc of blood and clot in her abdomen from a ruptured ectopic; I took out what was left of both Fallopian tubes. By now she should be menopausal and safe from that sort of misadventure.
December 13, 1977 My few days at the abortion clinic. The doctor is an OB/GYN who has also been doing abortions for 5 years. The office is attractive and comfortable. No one has ever been turned away for financial reasons. They will do abortions up to 14 weeks; after that they will refer the woman to someone who will do it later than that.
My first day; the receptionist gets a call at 8:30am. “Yes, Ma’am, I’m glad your mother did not have an abortion and I’m glad my mother didn’t either…No, we are not influenced by Communists. We don’t want to have anything to do with Communists…No, anyone who gets an abortion wants one. We don’t force people to have them.”
Every woman is personally counselled before the procedure. The woman is informed of the alternatives (having it and keeping it or giving it up for adoption, or having the abortion). The woman is asked why she wants it and is asked to sign a consent form. The procedure is explained in detail: the lab work (blood pressure, HCT (hematocrit); Rh typing and urinalysis); the actual abortion and the post session.
The woman is told what may happen as far as cramping: what to watch for; who to call if she has any questions. (Don’t go to the local Catholic hospital emergency room; women who have get pretty bad treatment.)
The first woman I go through with is young (about 20), unmarried, with her father. She is cool, a little afraid but very realistic. Everything goes OK with no problems. We talk before and after. She wants an apartment and is ready to leave home. Her father is surprisingly calm and is glad it isn’t “like the butcher shop years ago, f’ Chrissake!” We talk about Rhogam (she is Rh-negative), other methods of birth control, and so on.
The women are of all ages: young, middle aged, married with kids, single, divorced. Rich, middle class and poor. The reasons: “I’m not ready to start a family.” “I have kids and I’m getting too old.” “I can’t take being pregnant again.” How they got pregnant also varies: rhythm that didn’t work; a busted rubber; foam and no rubber; forgot the diaphragm; just got careless.
Some want to have kids later and feel it is the wrong time to start families. Some are from small towns, some from the big city. Catholic, Protestant, other.
Many of them are resentful of the Illinois legislature. Some think the representatives (mostly men) ought to try being pregnant. Most feel the option ought to be available. Everyone is glad to get it over with and swear they will never take chances again.
One woman today expressed frustration and anger at her husband, and at men in general who think birth control is always the woman’s responsibility. I’ve heard the reasons she says her husband gives and can’t believe people are still really like that. I feel for her because she is in a rotten position and needs some support. I listen and agree with a lot of what she says; she apologizes unnecessarily for “offending me.”
Next week I’m supposed to do the counseling myself (with an experienced counselor watching). This afternoon I will spend all night in labor and delivery. Strange world.
I wrote that almost forty-five years ago during my third year of medical school and a month shy of Roe v. Wade’s fifth anniversary. This year’s may be Roe’s last.
The physician, Dr. Richard Ragsdale, was a kind and compassionate man whose face resembled Lee Marvin. He would gently explain to the patient what would happen and always gave her the option of backing out. He would close his eyes when doing a bimanual pelvic exam, as if he was trying to mentally visualize the uterus. When the procedure was over, he would help her sit up, remind her of what to expect that was normal or concerning, and ask if she had any questions.
Then, as now, providing abortions wasn’t easy. Dr. Ragsdale’s clinic was firebombed. He was forced to do pregnancy terminations in a local hospital after the Illinois legislature adopted licensing regulations for outpatient clinics that were impossible to meet. Dr. Ragsdale sued the State in 1985 (Ragsdale v. Turnock, 625 F. Supp. 1212 (1985)). The Seventh District U.S. Court of Appeals ruled the Illinois regulations unconstitutional and the case continued to the Supreme Court but was settled in 1989. Dr. Ragsdale died in 2004.
I believe a few inconvenient and irrefutable facts:
First, and most important, women aren’t capable of inseminating themselves. The single requirement for an unwanted pregnancy is a willing dick with viable sperm. No politician has introduced legislation regulating accidental fatherhood, but maybe they should.
Second, preventing unwanted pregnancies can minimize the need for abortions but that requires, among other things, affordable and easily available contraception. GoodRx.com provides cheap oral contraceptives and Depo-Provera online. An IUD can run $500-$1300 but can last up to 12 years. The Colorado Family Planning Initiative provided long acting reversible contraception to low income women, cutting teen birth and abortion rates in half. Condoms cost about a buck each, less if bought in a box of 12 or more, but they won’t work if they are stuck in a wallet.
Sometimes a pregnancy implants somewhere outside the uterus and this “ectopic” pregnancy is life-threatening. The choice is removing the errant pregnancy or letting the woman die when the tube ruptures. When I was a resident we found a live fetus the size of a rice grain in a gestational sac hanging out the end of the Fallopian tube and no, we could not just move it to the uterus. Conservative thinking would potentially consider this an abortion.
Every birth control method, even permanent sterilization, has an inherent failure rate. Several years ago I saw a 42-year-old woman in a rural hospital’s Emergency Department complaining of a week of bleeding and abdominal pain. She’d had her tubes tied thirteen years previously but never thought she might be pregnant, but she had a positive pregnancy test. I found 1,300cc of blood in her abdomen from a ruptured ectopic pregnancy.
Preventing unwanted pregnancies also requires adequate sex education and the political will to ensure it happens. Countries with comprehensive sex education have far lower teen pregnancy rates than the United States. Determined teenagers will engage in sexual activity, regardless of adult pearl-clutching and sanctimonious bullshit, so get over it.
Finally, I don’t want someone telling me what to do, so no oneshould be telling any woman what to do!
“Since we all came from a woman, got our name from a woman, and our game from a woman. I wonder why we take from women, why we rape our women, do we hate our women? I think it’s time we killed for our women, be real to our women, try to heal our women, ‘cus if we don’t we’ll have a race of babies that will hate the ladies, who make the babies. And since a man can’t make one he has no right to tell a women when and where to create one.” ? Tupac Shakur
(I first wrote this 25 years ago. Perspective changes with time.)
I worked for a staff model HMO for nine years. Despite being a small cog in a sizeable organization, our Ob/Gyn department was like a second family to most of us. We knew about most of each other’s spouses (or ex-husbands). We shared our young kids’ accomplishments, antics and disappointments. We celebrated birthdays, expressed our condolences at the passing of elderly parents, and grieved together when a beloved young mother-to-be died in car crash. We had monthly department meetings at local restaurants after office hours, instead of trying to cram an agenda into a lunch hour.
Danni was the RN OB Intake Coordinator for our group. She was a gregarious soul with a kind heart and a good sense of humor. She spent an hour with each new mother-to-be at their first OB visit, talking about what to expect during pregnancy, what to do (eat healthy, wear a seatbelt and keep your appointments) what not to do (smoke, drink, anything blatantly stupid or dangerous). She was usually smiling, even when one of her appointments sorely tried her patience.
If she was having a particularly stressful day I would go to her office and wrap my arms around her. She said I gave great hugs; this was back when it wouldn’t trigger a visit from HR. I remember her colorful cable-knit sweaters under her lab coat and the warmth of her cheek against mine as she hugged me back, providing a brief respite from the day’s aggravations. Sort of like Mom telling you not to worry, that everything would be alright.
Danni suffered unrelenting physical pain from a tragic injury more than a decade earlier. We all knew about it, but to hear her talk it was more of an aggravation, something she’d learned to live with. Or maybe it was to deflect from the emotional torment she carried and of which only a few were aware.
I left the HMO in 1994; Corporate dissolved the staff model a few years later because “you cost us too much money.” Everyone found other jobs in town; Danni got a position with a local clinic. Our family had been torn asunder; we drifted apart and some connections withered from neglect.
I wandered for a couple of years, working in two different practices and a couple of locum tenens jobs before being hired to set up a practice in a small Southwestern town. I’d wanted to leave the long, gloomy Midwestern winters I’d endured for three decades and was trying to get out from under crushing but self-inflicted debt. (It hadn’t occurred to me that I was abandoning my kids as well, something I would later regret.)
In February, five months into the new practice, I flew Danni and Elizabeth, another former staff member, out to help train my nurse and receptionist. My new staff had no experience with an obstetrical practice, and I was used to someone else handling patient education. In retrospect, my support staff may not have been receptive to the intrusion but I needed the expertise.
Danni promised to send me forms and other information when she returned home. I called her several weeks later since I hadn’t received anything. She seemed distracted and vague but assured me she would “get around to it when I have time.” I should have suspected something was wrong. That was the last time I heard her voice. One evening she sent her daughter to spend the night with the neighbor next door. And ended her pain forever.
* * *
Linda, a nurse practitioner I worked with, called me early the next morning, sobbing. “Danni is dead!” “What happened?” “I don’t know. She had her daughter Katie stay at her friend’s house last night. She found Dani when she came home to get ready for school. I don’t know why, but they found a note.”
She continued to cry. “I remember she was suicidal when she left the clinic. I remember telling you she could never do that to Katy and you told me ‘Don’t bet on it.’ I don’t understand.” “I do,” I replied. “I understand all too well.”
I talked with Peg later that day and told her what had happened. “How are you handling all this?” “As well as I can.” “You know, I had a dream about you last week and I was afraid to tell you about it. You and I were talking and you told me you were going to kill yourself in the same tone you are using now. When I reminded you that you’d promised to keep going, you looked at me and said, ‘I was telling you what you wanted to hear.’ I heard the resignation in your voice. How could you do that?? Don’t you realize how much it would hurt everyone, including your kids???” “Yeah, but I wouldn’t be around to know it.”
Over the next 2 days we talked about suicide; Peg was very angry. “It’s so selfish! I don’t understand how she could calmly take her own life and leave her child with no one. There is always something else you can do.”
But for someone who has fallen into the abyss, such platitudes ring hollow. I know because I lived on the edge for almost 30 years and peered into the darkness many times. There comes a point when there is no more hope; when one has reached one’s limit of coping and can go no further. A point at which getting out of bed in the morning takes all the energy one has. There is nothing tangible to keep one moving, to make one want to take one more breath. Danni had reached her limit after years of constant physical pain and believing she had to go it alone. For all the people who cared and loved her, she finally could not continue.
The love of other people isn’t enough for some of us, because we don’t feel it is genuine or that we deserve it. On some level, I had long viewed that conditional “love” in the context of Billie Holiday’s song, God Bless the Child:
“Rich relations may give you A crust of bread and such You can help yourself But don’t take too much.”
Ironically, Nietzsche said, “The thought of suicide is a great consolation: by means of it one gets through many a dark night.” I survived many of those dark nights and ultimately determined I didn’t want to jump into the void.
A couple of days later I got an e-mail from Liz. “I got your message, thank you. I feel numb. I can’t believe it. I will never understand. Please, David, never do this!!!!!!”
* * *
Sarah was a 17-year old-gangbanger and troubled youth. Her father had also been a gang member, but he had turned his life around and tried to steer kids away from drugs, alcohol and living on the edge. Age and a stark reminder of mortality is often enough to trigger such an epiphany in adults, but teenagers either think they are immortal, or doomed to a life that can never change, so why bother.
Sarah was drunk the night she and some friends were playing chicken on the Interstate highway that ran north of town. They would lie on the white line while traffic approached at Autobahn speed, then run to the shoulder at the last moment. When Sarah’s turn came, she got up too late and was struck by a car. The local newspaper called it “an unfortunate accident” but some who knew her said she’d been severely depressed.
I went to the visitation with a family who had a troubled, angry 15-year-old daughter. I learned that when she threatened to run away from home, Sarah had talked her out it. “You don’t know how good you have it. You don’t ever want to live on the street!” Her friends and acquaintances, also “gangbangers,” appeared for the visitation, crying and holding on to each other for support.
I cried the tears I hadn’t been able to shed for Danni, and for those kids who felt they only had each other. I cried wondering why it took death to arouse family and friends from their oblivious slumber. Twenty-five years later I know some aren’t receptive to being helped, no matter how sincere the efforts.
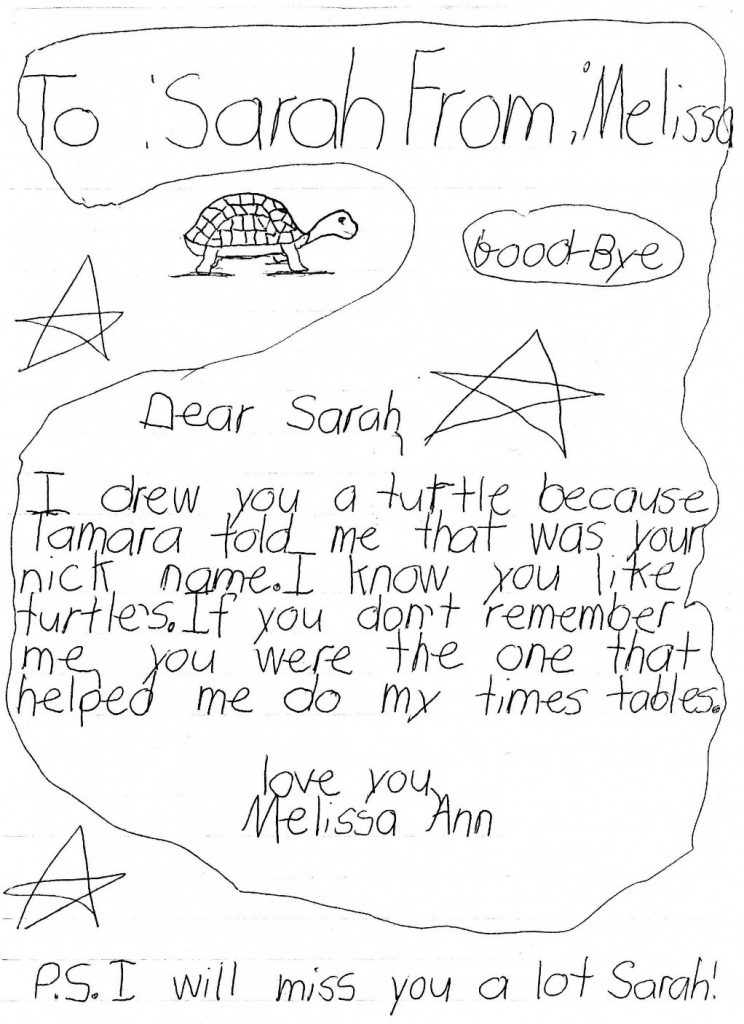
St. Mary’s Church was filled for the funeral. The gang members had printed T-shirts with “Turtle” (her nickname) over the left breast, and a memorial on the back: “In loving memory of Sarah Jo, 1980-1997.” During the eulogy Sarah’s cousin told the mourners, “If you love someone, tell them now. You never know when it will be too late.”
The procession to the cemetery stretched for 2 miles. After the priest finished, her friends released green and white balloons and sang for her. I couldn’t hear what they were singing. Instead, I heard a radio in the background playing “Forever Young” and then “That’s What Friends Are For.”
Melissa, 8 years old, wrote her own goodbye:
I held my 13 year old son and told him I loved him, even though I chewed his butt incessantly and tried to make him walk the straight and narrow. He blew it off, but deep inside I knew he understood and would always know that I loved him. I’d like to think my dad would have done the same.
A parent’s worst nightmare is having to bury a child long before his or her time.
A child’s worst nightmare is wondering what you did to make your parent commit suicide.