Why are men in commercials invariably portrayed as stupid (aside from the fact that many men are stupid)?
One local HVAC company runs two commercials several times a day. The first features a father with three adorable little girls, probably between five and ten, telling him that the house is falling apart. The youngest has a mischievous smile and undoubtedly has Daddy wrapped around her little finger. “Dad, the heat isn’t working!” “Dad, the toilet is backed up again!” Dad, this is a nice house, and you appear to have a lot of money, so why aren’t you taking care of it properly? Dad, looking dejected, says, “OK, I guess I’d better call someone. Hand me the phone book.” The youngest innocently replies, “What’s a phone book?”
After the voiceover tells the viewer about the company’s wonderful, prompt and competent service, the commercial ends with the little one sitting on Daddy’s lap. In one version, he says, “What would I do without you girls?” and the little one’s zinger is, “That’s a very good question.” Another ending has Dad asking, “How do you know about all this?” The little one responds “We’re girls, we know things!”
The other ad for this company is a version of “Is Timmy in the well?” The family dog is by the furnace and starts barking. “What is it boy?” *Bark bark!” “I changed the furnace filter.” *Bark bark bark!” “Do you think we need a new furnace?” You need a dog to tell you to get a new furnace, dumbass?
A rival HVAC company preys on the idea that men are unreliable when it comes to maintenance requests. Dad to adult daughter: You wanted me to look at your furnace? Husband to wife: You wanted me to check out the electrical problem? Women’s answer: You took too long so I called PQR company! Men’s predictable answer: OK, so it’s done. (Good, because I didn’t wanna do it in the first place. Took you long enough to get the hint, eh?)
A young suburban homeowner wants the insurance protection of that company whose logo is a red roof, but he’s obviously too cheap to pony up, so he’s jerry-rigged a wooden roof outline over his house and is painting it red. Two famous Canadian guys from a famous Canadian house show tell him, “That’s not how it works.” Well, DUH!
Speaking of insurance, there’s that company whose spokesman, a PhD (Phony Doctorate) life coach who says, “We can’t keep you from turning into your parents.” Said by the guy wearing a knit sweater vest from the 1980s. Then they give examples of egregious parent-like behavior: • Three guys giving a fourth unsolicited advice on building a fire in the backyard firepit. • Guys obsessed with the weather, calling each other with updates. • Obsessive host hovering around guests at a backyard cookout; the husband is wearing an apron with a “Kiss-the-Cook” type message. • A guy at a gas station striking up an unwanted conversation with another guy because he can’t stand the silence.
Now, I’m a parent and a grandparent and I don’t know anyone who pulls this shit. These characters appear to be middle-class white suburbanites, but I live in a nice suburban neighborhood and the only person I talk to is the guy across the street and only when we’re both outside. I might text the local relatives if there’s a tornado warning, or my sister-in-law to make sure their basement isn’t flooding when we have torrential rain, an occurrence that has become far less frequent with climate change. I’ve never seen guys talking to each other at a gas station. I have a nondescript, Southwestern motif apron, and a vinyl blood splatter-proof Dexter apron my daughter bought me. My grill conversation is:
“What kind of cheese do you want on your burger?” “How burnt do you want your hot dogs?” “How about you move the hell away from the patio door, or help me bring this stuff inside instead of just running your mouth at the kitchen counter?”
Maybe it’s just the curmudgeon in me, but I think we deserve a little more consideration by whatever idiots write ad copy.
I really hate what our healthcare system has become after Corporate America took over!
I had a colonoscopy in 2021 during which my gastroenterologist, Benny Thomas removed a tubular adenoma, a type of precancerous polyp, along with three other polyps. I’ve had internal hemorrhoids for as long as I can remember, so occasional rectal bleeding has never been surprising. However, over the past few weeks I’ve had much more frequent bleeding, sometimes with little clots, which would be less concerning had I not had radiation for prostate cancer nineteen months ago. Radiation treats cancer but can also trigger new cancers.
All the large health care groups where I live use MyChart®, an electronic health record (EHR), which supplanted the old paper charts. I suspect I’m not the only one who has a love-hate relationship with it. Patients can look at test results and notes from office visits, make appointments online, and, most importantly, pay their outstanding bills or copays before office visits. They can communicate easily with their health care providers or authorized designee (read: nurse) through the messaging app. Or so I assumed.
My GI guy is affiliated with Pretentious Healthcare Network (PHN), not with my usual stable of providers at the eternally aggravating Suburban Medical Group (SMG). Ruthless University Bastards (RUB) is another predatory group in the area that has an unfortunate habit of gobbling up hospitals and stripping them of “frivolous” amenities the previous owners provided to make the lives of patients and staff a little more pleasant, all in the name of “fiscal responsibility.”
I signed into PHN’s MyChart to make an appointment, but the system thought I was a new patient, because my colonoscopy was a little more than three years previously. (Three years seems to be the magic cutoff; time to cull the herd.) Nope, you’re 2 months too late; too bad, so sad. Dr. Thomas’ first available appointment was in six months, and I really didn’t want to start over with a new physician, so I called “the office.”
Now, when I was a teenager growing up in small-town Illinois, accessing health care was far less complicated. My mother would call the doctor’s office and talk with his nurse (in the 1960s most physicians were men) who would take a message, put my mother on hold, talk with the doctor, and return with instructions to come to the office or sit tight. During the night, the doctor’s wife answered the phone so he could sleep, and she would tell you to go to the ER or take two aspirin and call the office in the morning.
Not anymore, Monty. There is no way in hell I can call any office directly. Instead, there is one phone number for all the physicians in a specific practice (internal medicine, pediatrics, cardiology, etc.), or, in PHN’s case, Specialty Care, which includes a host of specialists lumped together. Physicians and nurses, people who do actual work, are shackled by the system. We are all “only pawns in game of life.” It’s another reason I’m glad I retired.
I called Specialty Care on Monday morning, and the system immediately hung up. That is probably because the people who ignored their problems over the weekend call on Monday. I thought I’d be more successful waiting until Tuesday morning after the crowd thinned out.
I connected after a couple of rings:
“Thank you for calling Pretentious Healthcare Network’s medical specialties group. If you are having a life-threatening medical emergency, please hang up and dial 9-1-1 immediately as we’re not gonna waste time resuscitating your sorry ass over the phone. Now, what do you want? Are you calling about an appointment or test results?” Yes “Sorry, I didn’t understand that. If you are calling to make, cancel or reschedule an appointment, say ‘appointment.’ ” Why the fuck didn’t you say that in the first place? You asked me a yes/no question!!!
After saying “appointments” a few times and hearing “I didn’t understand that” I got connected to a live human. I explained my situation: I was an established patient; I’d had significant rectal bleeding for the past few weeks; I’ve had precancerous polyps taken out in 2021 and I had radiation in 2023. Dr. Thomas’s first available appointment on MyChart was in six months. She then asked the questions I needed to answer to continue my quest:
“What is your name?” “What is your date of birth?” “What is your address?” “What is the air-speed velocity of an unladen swallow?”
Satisfied with my responses, she said she’d relay this to the doctor’s nurse who would then call me back.
I got a call three hours later from Gracie, Dr. Thomas’s nurse. I repeated my story. Did she not understand the message from the gatekeeper or is she testing me to determine if there are any discrepancies? I explained twice that I had radiation therapy which ended in March 2023.
“You need to get a CBC.” “I had one a few weeks ago.” “I don’t see it here.” “You won’t because I get my bloodwork done with an outside service.” “Do you have the results?” “Yes, let me pull it up on my computer. Would you like me to send you a copy?” “That would be great! Can you use the messaging app on MyChart?”
I started using an online laboratory service, DirectLabs, in 2007 when I was an independent contractor with high-deductible insurance. I ordered the tests I wanted and paid online; the company would send me a requisition approved by one of their physicians. Then I would made an appointment at any of Quest Diagnostics locations, get my blood drawn and receive my results in a day or two. It was far cheaper and more convenient than getting blood tests from one of the local providers.
I still use DirectLabs every year. I can get the Comprehensive Wellness Profile for $97; it includes: • Comprehensive Metabolic Profile (CMP) (blood glucose, kidney and liver function tests and electrolytes) • Complete blood count (CBC) • Lipid profile (cholesterol and triglycerides) • Thyroid Stimulating Hormone (TSH) • Iron, uric acid, and phosphate And there isn’t an additional $20 charge just for sticking a needle in my arm!
I signed into MyChart only to discover that I couldn’t send a message and attachment to her because “There are no providers you can contact.” I couldn’t reply to the last message exchange between me and Dr. because “This message is too old to respond to.” Well, fuck you very much. So, being resourceful and proactive, I printed the report and drove to the office which was only a little over seven miles away but took half an hour because the main drag was backed up like rush hour for no apparent reason.
Dr. Thomas’s office had moved to another part of the facility since my last visit. The entry from the parking lot ended at an intersection – left for the Emergency Room, right for outpatient services. I recognized the area as I’d waited here when I had cataract surgery last Halloween. My eye caught a sign for “Specialty Care Group” on the right, but it was every specialty except the one I needed. I walked farther into the area and eventually found a directory on the wall behind me.
The office was on the second floor. I got into a dimly lit elevator with three other people. The four tiny, recessed lights in the ceiling made the car feel like a sleazy city alley. I almost asked the other people if we should be afraid of being mugged but thought better of it.
I found the office and asked the receptionist if Gracie was still around (she also works in another office across town).
“Yes, but I don’t know if she’s in today.” “I know she’s in because I just talked to her. Would you give her this?”
I handed her my report and left.
Gracie called me back while I was driving. I couldn’t answer so I waited until I got home; she left a message asking me to call her back. That meant going through the whole process yet again: waiting in the queue, “call 9-1-1, blah, blah, blah;” “appointment, dammit;” explaining to the sweet young thing; getting put on hold while she tracked down Gracie.
“I talked with Dr. Thomas. He can see you at 4:40 p.m. tomorrow but he wants you to get another CBC before he sees you.” “Why? It’s only been a couple of weeks.” “Have you been light-headed or dizzy?” “No, I’m not anemic. You know I’m a physician?” “Yeah, I kinda assumed that. But he wants another CBC.” “Well, I’m not gonna drive back out there and waste another hour. Is there any place closer?” “You live in Lombard? There’s one on Main Street in Lombard.” “Is it in the sleep center?” “No, it’s farther down, near downtown.” (“Downtown” is a misnomer: it’s what the town used to be 100 years ago and about eight blocks long. The rest of the city is suburban sprawl.) “Oh, I know; across from the Dairy Queen!” “That’s it.”
The location was open until 7:30 p.m., at least according to Google. There’s an urgent care in the building and one would assume if they see patients until 7:30 p.m. that the lab would also be open should anyone need blood work. And one would be wrong.
I planned on Peg and I going there after she was finished working and before we went out to dinner. We arrived at 5:30 p.m. but the receptionist told me the lab closed at 5:00 p.m.. As we walked out, a couple in scrubs, presumably from the outpatient surgery center, said the lab closed at 4:00 p.m.. Irrelevant, since I was too late and therefore fucked.
The next morning Peg woke me up, all excited. She remembered the urgent care just up the street, a former bank, is one of PHN’s and has a drive-through lab open 6:30 a.m.- 6:30 p.m.. Technically, it’s in the next town but a lot closer than the Dairy Queen location.
It was a great setup! They had enclosed three former drive-through banking lanes with glass and aluminum garage doors. I called the number on the stop sign outside the lanes, gave someone my information, and waited for a door to open. Then I pulled in and stopped by the phlebotomist and her equipment cart. The area is climate-controlled judging by the thermostat on the wall and she wasn’t wearing a jacket (the outside temperature was about 45°). She asked me to open the door and stick my arm out. A couple of minutes later my blood had been drawn, the tube properly labeled, and I was out the door.
I went to vote early, picked up breakfast from Sonic, came home and logged on to my computer. I saw an e-mail from PHN asking me to complete online check-in to save time. It’s one of the few benefits of EHR’s. No more sitting around with a clipboard and multiple pieces of paper, trying to list your drugs on single spaced lines. I did all that and continued through email.
“There is a message from your provider’s office.” The message: “Appointment cancelled. Time: 4:20p.m..” WTF? I called the main number and went through the queue YET AGAIN. Apparently, someone had made my appointment for 4:20p.m., cancelled it and moved it to 4:40p.m.
What might have happened if I was just a regular old person who didn’t think of pursuing this? “Well, they cancelled my appointment, so I won’t go and hope they will call me back to reschedule.”
We finally saw Dr. Thomas, a man whose rugged face and thick grey hair would make him perfect for a soap-opera physician.
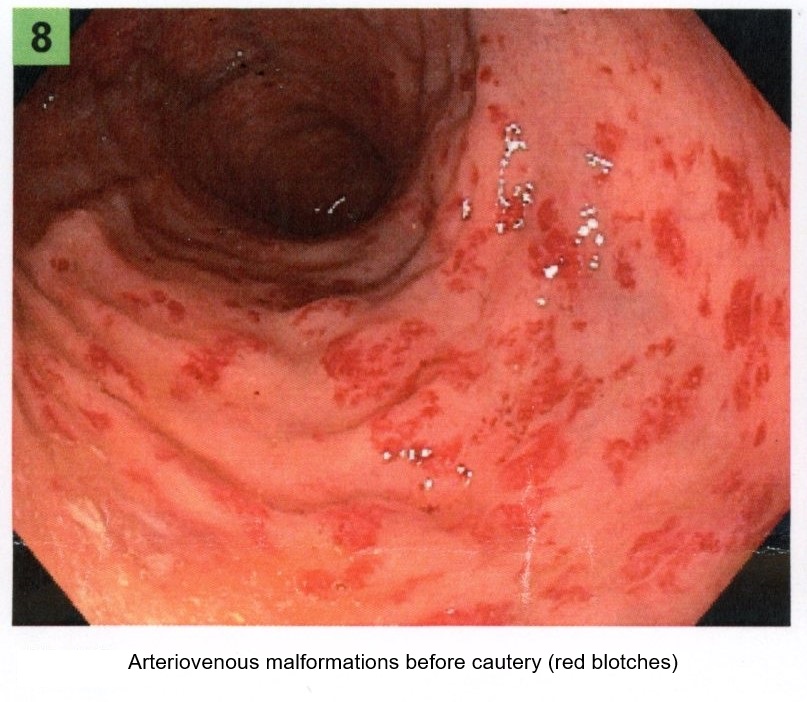
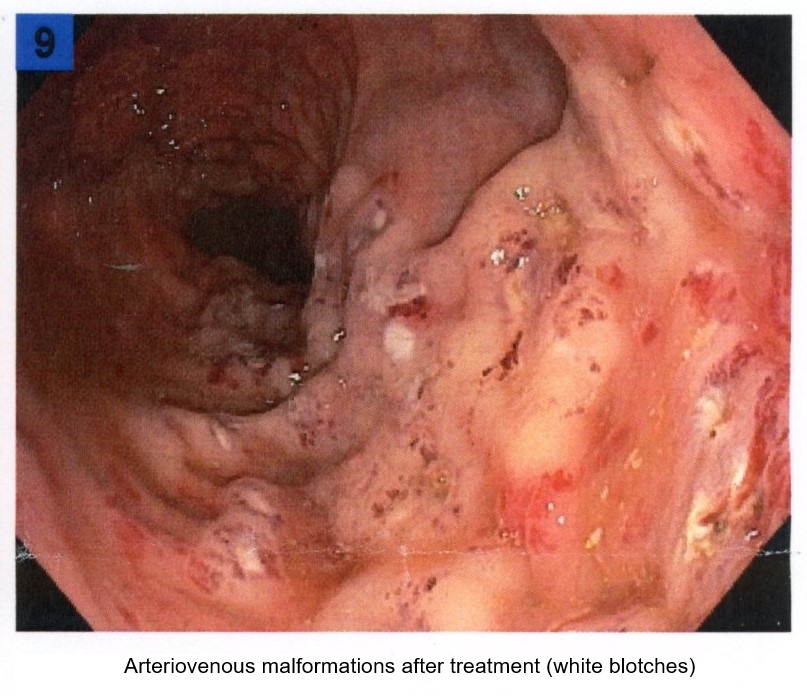
“I understand you’re having rectal bleeding.” “Yeah, it started a couple of months ago, but it’s become a lot more frequent, sometimes every day. Since I’ve had pelvic radiation, a new cancer was the first thing that popped into my head.” “We see this a lot. You probably have AVMs – arteriovenous malformations – which are like little spider veins you see on the faces of old people. They are fragile, easily broken and likely what’s causing your bleeding. This can happen up to two years after radiation.” (I don’t remember my radiation oncologist mentioning this.) “We can cauterize them with an APC (argon plasma coagulator) but since that requires a colonoscopy and you’ve had adenomatous polyps, we should just look at your entire colon.” “OK, fine by me.”
He asked me to change into a gown so he could do an external anal exam, then he left the room. I could have just dropped my pants and bent over like I did during prostate exams, but whatever. When he returned he had a quick peek, which seemed hardly worth the trouble.
“It looks good. I’ll have my nurse check the schedule and find a date.”
I wasn’t prepared when his nurse returned and asked, “Would Friday (two days later) work for you?”
I had a deer-in-the-headlights moment and didn’t know what to say. Bowel preps are time-consuming and annoying. Normally one has to start with altering the diet about five days before the procedure. I reluctantly agreed, having forgotten a dinner engagement on Saturday.
Ah, but there was another fly in the ointment that would delay things. The practice puts the burden of obtaining preauthorization for procedures on the patient. Fortunately, being married to someone working for the company that provides your insurance has its benefits. Peg called and talked with the woman who was a great help when I was going to have radiation therapy in 2023.
The healthcare coding system is the bane of physicians’ existence. We need to have an International Classifications of Disease (ICD-10) diagnosis code as well as a Current Procedural Terminology (CPT) code for the procedure. There’s also the Healthcare Common Procedure Coding System (HCPCS), pronounced “Hick-Picks” that the Centers for Medicare and Medicaid Services (CMS) requires. This nonsense is yet another reason I’m happy to be out of the biz.
Our insurer doesn’t require preauthorization for a diagnostic colonoscopy, but it does for planned APC. (Pop quiz: what does APC stand for?) I returned to the phone queue, got Dr. Thomas’s nurse and went round and round over the coding, trying to get her to understand that if I didn’t get preauthorization if needed, I’d potentially be on the hook for the entire charge plus a $250 “no-no-bad-dog” penalty. The fact that MyChart prevented me from replying to her messages just added to the aggravation.
So, I took the bull by the short ones and searched Google. I found the “2023 Coding & Payment Quick Reference” put out by Boston Scientific which had a code for “Colonoscopy, flexible; with control of bleeding, any method,” and sent it back to the nurse. The next morning, I was roused from my slumber at 8:00 am (no, I am NOT a morning person!). The doctor was happy with using that code and so was the preauthorization person. He also had a cancellation for the following Thursday, which worked out for us.
I ran into a minor snafu at the pharmacy with the bowel prep. The main ingredient in all bowel preps is polyethylene glycol (PEG-3350), the stuff in Miralax. Industrial-strength preps like Nu-Lytely (Gavalax-N is the generic), add sodium and potassium chloride, and sodium bicarbonate to minimize the electrolyte loss and potential cardiac complications of flushing one’s bowel with a gallon of fluid.
However, the most reviled of modern bowel preps is Go-Lytely, an evil concoction with sodium sulfite added to the other electrolytes. The result is something that smells and tastes like rotten eggs and is very salty. It’s one of the reasons most people hate bowel preps. The pharmacy wanted to give me Go-Lytely, but it appeared that Nu-Lytely had also been prescribed, so I took the latter.
The prep went relatively well, although chugging down half a gallon of cold solution that tastes like flat lemon-lime soda in less than three hours is a challenge. It might have been easier if the outside temperature was in the 90s instead of mid 40s. I warmed up some apple juice with a cinnamon stick to ward off the chills.
The Endoscopy Center called me mid-afternoon to tell me my procedure would be at 1:15 p.m.. I had to drink the other half gallon of solution starting six hours before getting the tube, so at least I could sleep all night. Squirting warm, yellow liquid out your butt isn’t pleasant, but it could be so much worse.
We got to the Endoscopy Center a little before noon. I had my driver’s license, my Medicare card, and my insurance card in hand, but all the receptionist wanted to know was my birth date and home address. The waiting area was in the hall and seating was limited; we ended up in a couple of chairs just outside the double doors leading back to the suites.
About twenty minutes later a nurse in scrubs came through the door and said, “Harold.” A woman next to her yelled, “Hank! HANK! Get back here; they’re calling you.” Hank had gotten a little bored and wandered down the hall for no apparent reason, much to his wife’s irritation. I heard her say to the nurse, “Tell him he can’t go roller skating tonight!” (My postoperative instructions cautioned against making critical decisions and operating any kind of machinery, “including kitchen appliances.”)
My turn came sooner than I expected, but was still a lot later than it should have been. A sweet young nurse named Cassidy, probably shy of thirty years, ushered us into the same room Peg had occupied when she had her colonoscopy, sans sedation, several years ago. I knew the drill very well: strip completely, put on the patient gown, open to the back, get on the cart and wait for her to put on EKG leads, take my blood pressure and pulse oximetry, and then start an IV.
Sometime during all this Peg mentioned I was a physician (after thinking Cassidy was talking to me like a five-year-old), and she perked up.
“What kind of physician?” “Obstetrics.” “I was an obstetric nurse at Holy Smokes Hospital!” “How long ago?” “About four years” “I worked there in 2010.” “I graduated high school in 2014!”
OK, so I could be either your father or grandfather. Thanks a lot.
Several minutes later Cassidy returned to tell us things were running late. Dr. Thomas was finishing one procedure; he had another, shorter procedure, before it was my turn. She left and I closed my eyes to ward off the boredom.
Then I heard a procession in the hall with someone yelling, “Frank. FRANK! We’re done and we’re going back to your room. Stop trying to get off the cart!” (Frank growled something unintelligible, which faded as they passed).
Finally, I saw Dr. Thomas, who asked us if we had any questions, followed by the CRNA who went over my medical history. Peg and I both stressed that I had a paradoxical reaction to benzodiazepines like Versed, which, along with fentanyl, is often used for sedation. She assured us they only used propofol. A few minutes later one of the OR nurses came to take me to the room.
“Wait a sec. I should go to the bathroom one last time.” “Number one or number two”? “Number one…what?” (Do I look like I’m a fucking kindergartener???) “If it’s number two, don’t worry. We suck everything out anyway.” (I’ll keep that in mind for next time.)
I went into the restroom just across the hall and then climbed back onto the cart before she wheeled me into the procedure room.
Now, I’ve mentioned before how I find anesthesia fascinating. The conscious brain is disconnected from the rest of the brain and body, and it feels like time stops. This time I remember the dark curtain falling as they pushed the propofol. Hasta la vista; meet you on the other side.
IV sedation also removes inhibitions until the consciousness fully recovers. Apparently, I was a potty mouth when I returned. It started when the nurse was trying to adjust my blood pressure cuff and get me off my left side, where I’d been lying since the procedure began. Peg relayed my comments after I’d regained some semblance of coherence:
“This is bullshit! Pardon my French.” “They fucking zapped my ass.” “That guy on the cart who tried to do a runner was an asshole.” “Propofol is fucking great!”
I felt bad for exposing Cassidy to such profanity, but Peg assured me I was probably the least of her problems. An able-bodied man in the next room, waiting for his wife to return, was too fucking lazy to go to the bathroom across the hall and instead, peed into a urinal he found in the room. The problem was his aim sucked, and the poor nurse was left to wipe his pee off the floor, then empty the urinal in the bathroom because he was too lazy to do it himself.
I still think I should send Cassidy a note with an apology.
As suspected Dr. Thomas found several arteriovenous malformations, the source of my bleeding. Here are before and after pictures.
He also snagged four pre-cancerous tubular adenomas. I think I’m predisposed to other cancers, given I’ve already had prostate cancer and pelvic radiation. So now I’m on the three-year plan. I’ve already set a notification to call the GI office before the end of three years, so I don’t have to repeat this bullshit.
I had a phone visit with my radiation oncologist two months later.
“You should really tell your patients about arteriovenous malformations.” He paused for a moment. “I developed rectal bleeding and…” “Oh, I thought you were talking about brain AVM. Yes, this is radiation proctitis and it happens in about 1% of patients.”
(Yeah, well that would have been nice to know).
It’s been seven months, and I haven’t had any more bleeding. But my PSAs are still rising, so I’ll be seeing the radiation oncologist again next month. Good times.
December 13, 1977 My few days at the abortion clinic. The doctor is an OB/GYN who has also been doing abortions for 5 years. The office is attractive and comfortable. No one has ever been turned away for financial reasons. They will do abortions up to 14 weeks; after that they will refer the woman to someone who will do it later than that.
My first day; the receptionist gets a call at 8:30am. “Yes, Ma’am, I’m glad your mother did not have an abortion and I’m glad my mother didn’t either…No, we are not influenced by Communists. We don’t want to have anything to do with Communists…No, anyone who gets an abortion wants one. We don’t force people to have them.”
Every woman is personally counselled before the procedure. The woman is informed of the alternatives (having it and keeping it or giving it up for adoption, or having the abortion). The woman is asked why she wants it and is asked to sign a consent form. The procedure is explained in detail: the lab work (blood pressure, HCT (hematocrit); Rh typing and urinalysis); the actual abortion and the post session.
The woman is told what may happen as far as cramping: what to watch for; who to call if she has any questions. (Don’t go to the local Catholic hospital emergency room; women who have get pretty bad treatment.)
The first woman I go through with is young (about 20), unmarried, with her father. She is cool, a little afraid but very realistic. Everything goes OK with no problems. We talk before and after. She wants an apartment and is ready to leave home. Her father is surprisingly calm and is glad it isn’t “like the butcher shop years ago, f’ Chrissake!” We talk about Rhogam (she is Rh-negative), other methods of birth control, and so on.
The women are of all ages: young, middle aged, married with kids, single, divorced. Rich, middle class and poor. The reasons: “I’m not ready to start a family.” “I have kids and I’m getting too old.” “I can’t take being pregnant again.” How they got pregnant also varies: rhythm that didn’t work; a busted rubber; foam and no rubber; forgot the diaphragm; just got careless.
Some want to have kids later and feel it is the wrong time to start families. Some are from small towns, some from the big city. Catholic, Protestant, other.
Many of them are resentful of the Illinois legislature. Some think the representatives (mostly men) ought to try being pregnant. Most feel the option ought to be available. Everyone is glad to get it over with and swear they will never take chances again.
One woman today expressed frustration and anger at her husband, and at men in general who think birth control is always the woman’s responsibility. I’ve heard the reasons she says her husband gives and can’t believe people are still really like that. I feel for her because she is in a rotten position and needs some support. I listen and agree with a lot of what she says; she apologizes unnecessarily for “offending me.”
Next week I’m supposed to do the counseling myself (with an experienced counselor watching). This afternoon I will spend all night in labor and delivery. Strange world.
I wrote that almost forty-five years ago during my third year of medical school and a month shy of Roe v. Wade’s fifth anniversary. This year’s may be Roe’s last.
The physician, Dr. Richard Ragsdale, was a kind and compassionate man whose face resembled Lee Marvin. He would gently explain to the patient what would happen and always gave her the option of backing out. He would close his eyes when doing a bimanual pelvic exam, as if he was trying to mentally visualize the uterus. When the procedure was over, he would help her sit up, remind her of what to expect that was normal or concerning, and ask if she had any questions.
Then, as now, providing abortions wasn’t easy. Dr. Ragsdale’s clinic was firebombed. He was forced to do pregnancy terminations in a local hospital after the Illinois legislature adopted licensing regulations for outpatient clinics that were impossible to meet. Dr. Ragsdale sued the State in 1985 (Ragsdale v. Turnock, 625 F. Supp. 1212 (1985)). The Seventh District U.S. Court of Appeals ruled the Illinois regulations unconstitutional and the case continued to the Supreme Court but was settled in 1989. Dr. Ragsdale died in 2004.
I believe a few inconvenient and irrefutable facts:
First, and most important, women aren’t capable of inseminating themselves. The single requirement for an unwanted pregnancy is a willing dick with viable sperm. No politician has introduced legislation regulating accidental fatherhood, but maybe they should.
Second, preventing unwanted pregnancies can minimize the need for abortions but that requires, among other things, affordable and easily available contraception. GoodRx.com provides cheap oral contraceptives and Depo-Provera online. An IUD can run $500-$1300 but can last up to 12 years. The Colorado Family Planning Initiative provided long acting reversible contraception to low income women, cutting teen birth and abortion rates in half. Condoms cost about a buck each, less if bought in a box of 12 or more, but they won’t work if they are stuck in a wallet.
Sometimes a pregnancy implants somewhere outside the uterus and this “ectopic” pregnancy is life-threatening. The choice is removing the errant pregnancy or letting the woman die when the tube ruptures. When I was a resident we found a live fetus the size of a rice grain in a gestational sac hanging out the end of the Fallopian tube and no, we could not just move it to the uterus. Conservative thinking would potentially consider this an abortion.
Every birth control method, even permanent sterilization, has an inherent failure rate. Several years ago I saw a 42-year-old woman in a rural hospital’s Emergency Department complaining of a week of bleeding and abdominal pain. She’d had her tubes tied thirteen years previously but never thought she might be pregnant, but she had a positive pregnancy test. I found 1,300cc of blood in her abdomen from a ruptured ectopic pregnancy.
Preventing unwanted pregnancies also requires adequate sex education and the political will to ensure it happens. Countries with comprehensive sex education have far lower teen pregnancy rates than the United States. Determined teenagers will engage in sexual activity, regardless of adult pearl-clutching and sanctimonious bullshit, so get over it.
Finally, I don’t want someone telling me what to do, so no oneshould be telling any woman what to do!
“Since we all came from a woman, got our name from a woman, and our game from a woman. I wonder why we take from women, why we rape our women, do we hate our women? I think it’s time we killed for our women, be real to our women, try to heal our women, ‘cus if we don’t we’ll have a race of babies that will hate the ladies, who make the babies. And since a man can’t make one he has no right to tell a women when and where to create one.” ? Tupac Shakur
We switched to Sempiternity because Awesomely Terrific and Tremendous’ internet kept going out, but what we gained in reliability we lost in signal strength to our upstairs offices. The guy who installed our cable and network recommended the new Sempiternity Capsule, a Wi-Fi extender that is supposed to “help eliminate dead spots,” augmenting the pitch with buzzwords like “consistent,” “seamless,” “performance,” and “enhanced.” The Capsules are “optimized” to work with the Sempiternity Grand Portal, meaning you are SOL if you bought your own router to avoid the rapacious rental fee.
Amazon sells the Sempiternity Capsule for $189 each. Sempiternity sells one Capsule for $119 ($199 for two) but charges an outrageous fifteen bucks for “shipping and handling.” One might figure going to the local retail store would be quicker and easier.
And one would be wrong.
I walked in and there was barely three feet between the front door and the long desk planted like a TSA checkpoint, behind which was an employee (excuse me, “customer service representative). He instructed the man in front of me to move into the corner to my right, where another rep was dealing with a woman, then turned back to me.
“What can I help you with today?” “I want to pick up a Capsule.” “Ok, can I have your first name and first initial of your last name?” “David. R.” “Ok, David, have a seat and someone will be with your shortly.”
I spotted nine customer service desks occupied by only five representatives. (Eventually, two more reps showed up.) There was least a dozen more people trying (and failing) to maintain social distancing in the two seating areas (*cough* holding pens *cough*). The middle one had several leather chairs while the one near the back had two benches with no backs, sitting perpendicular to each other. A young man with a tablet mingled with the people lucky enough to score a chair, assuring them someone would eventually call their names.
I took a seat on an uncomfortable bench with no back, across from a Hispanic man and his son. A large TV was silently running an episode of the Chopped Star Power tournament with Dorothy Hamill and three people I didn’t recognize. I couldn’t identify where the crappy bass-heavy music was coming from. I assumed this was going to take a lot longer than I’d hope, so I started the stopwatch on my phone.
Like most media stores, this one was built more for showcasing merchandise than creature comfort and/or efficiency, and I noted a few problems:
Sound bounces around in an open setup and the ambient background noise increase exponentially with each additional body.
The customer service reps were calling out names in uniformly inefficient decibel levels.
Many of the customers were old people with bad hearing and the aforementioned crappy music didn’t help.
As I looked around, I spotted the Capsules on shelves next to the TV. I grabbed one and returned to my seat, which was now occupied by a trio at the other end. Seriously, folks, there is no need to travel in packs during a pandemic, even if we are nearing the end.
No one responded to a few of the names called; I assumed they’d become frustrated with the wait and left. By now I’d been sitting there for twenty minutes, but I didn’t want to leave and have to start all over another day.
Finally, a very nice woman and one of the later arrivals called my name. I walked over to her station and put the Capsule on her desk.
“You want to return this?” “No, I want to buy it.”
She started futzing with a tablet, even though there was a computer screen on the desk. She scanned the box’s barcode, then started muttering to herself. A few minutes later she asked a sweet young thing with two-inch fake fingernails for help. Then they both started muttering.
“I’ve been working here a long time, but they just switched to using tablets and we’re all trying to get used to them.”
Great.
After more muttering and futzing, she asked me for my credit card, swiped it through the port on the tablet and I thought we were done.
“Do you want a paper receipt, or have it emailed?”
“Email would be fine.” (I HATE paper receipts because of the clutter and the propensity for disappearing.
“What’s your email address?” “It should be linked to my account.” “Uh, we can’t get to it through our system.” For fuck’s sake!
“Give me your tablet and I’ll type it in. It will be a lot faster than spelling it for you.” Some people don’t know what a curmudgeon is and those who do think I’ve misspelled it. No, I spell it that way because “curmudgeon” was already taken, presumably by a kindred spirit.
Thirty six minutes and twenty seconds later I was in my car heading home.
One activates the Capsule with the Sempiternity phone app. (I’m not sure what someone without a smart phone is supposed to do, since Sempiternity won’t send out a tech just to set it up.) The YouTube setup video says it’s supposed to be simple:
Make sure the phone’s Bluetooth is on and searching.
Plug in the Capsule and hold the phone within six inches.
After the Capsule is recognized, wait up to five minutes for the system to bring it online.
So, went up to our second floor bedroom, plugged the Capsule in and waited.
Nothing happened.
Well, almost nothing. A tiny light in the Capsule turned blue, then green and started blinking. A circle of continuously changing hue ran around the “Connecting the First Capsule” graphic for 10 minutes before the light changed to blinking white and the app said, “Your Capsule is not online.” I tried again using an outlet in the hallway. Nothing.
I went downstairs to the kitchen and tried again. No dice. Finally, I plugged it in to an outlet in my family room about six feet from the Grand Portal.
Nope.
I shouldn’t have been surprised. Our upstairs cable box kept turning itself off every ten minutes about an hour after the installation guy left back in November, prompting a visit to the Sempiternity store. I waited a couple of days for my patience to renew.
I thought arriving ten minutes before the store opened would avoid the crowd. Silly me. There was already a half-dozen people milling around in the cold, waiting for the door to unlock. I joined them rather than find myself even further back of the line.
The customer service dude took my name. I grabbed one of the more comfortable chairs this time and restarted the stopwatch, making a silent bet with myself on how long this would take.
Someone called “David?” after about ten minutes.
I walked over to the desk, Capsule in hand and said, “I want to return this. It doesn’t work and yes, I tried several times. I don’t want a replacement.”
“Ok, well, let me take care of that for you.”
He took the box and scanned the barcode with his tablet. Frowning, he tried again. He turned the box over in his hand, possibly looking for another barcode (which didn’t exist). He called one of the other customer service dudes and they huddle for a few minutes.
“Uh, I can’t do refunds with the tablet. I have to use that computer over there,” which was tied up with another customer.
Ah, the irony. Corporate sets everyone up with tablets that should do everything but can’t process refunds.
This time only took 20 minutes, minus eight for standing in line outside.
It should be intuitively obvious but remember customer service reps are just poor bastards trying to earn a living. Most of them are nice and try to be helpful, even when dealing with abusive assholes. Taking your frustrations out on them by yelling, screaming or indignantly asking to see the manager isn’t helpful. They aren’t responsible for long waits and uncomfortable seats. It’s likely none of the corporate types who design retail outlets have ever set foot inside of one, let alone as a customer. So be polite, say “thank you,” and count your blessings if you work for a company that truly gives a shit about their employees.
Afterword: I ordered a tp-link Wi-Fi 6 Range Extender from Amazon for $70. The instructions were simple: 1. Plug in the extender in an outlet near the router. 2. Download tp-link’s Tether app and create an account. 3. Tap + in the app to connect with the router. If wi-fi LED is solid blue, you’re good. 4. Plug the extender in at the desired location. 5. Enjoy your extender.
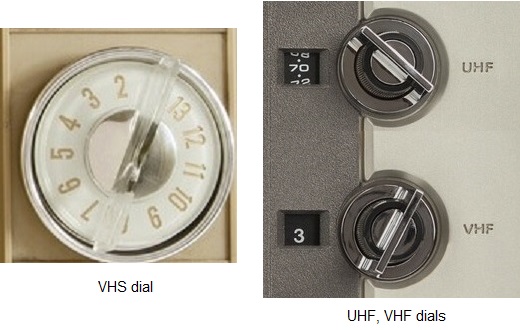
We lived in Bisbee, Arizona from the late 1950s until the mid-1960s. The nearest television stations were 100 miles away in Tucson, far beyond the range of “rabbit ears” antennas, so rural communities like ours had Community Antenna Television (CATV). Several towers erected on Juniper Flats, a plateau on the mountain northwest of town, captured VHF (Very High Frequency) signals and distributed them to houses through coaxial cable. A small adapter allowed one to connect the cable to the two antenna terminals on the back of the TV and voilà! A great picture, no snow, no ghosts and no need to fiddle with a UHF ring tuner (that “U” on the dial). Everyone watched the same shows, and we liked it, dammit!
Rabbit ears antenna
By 1970 cable had became more popular as many households ditched their antennas. The shift happened despite early FCC meddling and intimidating ads the networks aired in movie theaters decrying the evils of “pay TV.” Yet Home Box Office successfully launched in 1972 and has been with us for fifty years.
Televisions changed over the next several years. Manufacturers added a separate UHF dial as more channels became available, eventually replacing both dials with a single internal tuner. Cable connected directly to a coaxial port. Small children served as early channel changers, performing double duty as antenna adjusters. Actual remote controls evolved from wired (Zenith’s “Lazy Bones”) through primitive wireless (Zenith’s “Space Command” and Magnavox’s “pig whistle”) to ultrasonic and finally infrared.
Videotape became popular in the 1980s but with only one port available, the cable had to be routed through the player/recorder and then to the television. One tuned to Channel 3 or Channel 4 to watch a videotape. Later televisions had two coaxial ports and early game systems supplied a box switch.
An alphabet soup of basic cable networks – CNN, TBS, TNT, CBC, TLC, VH1 and others – proliferated during the 1980s. A smarmy meme noting MTV’s 40th anniversary read, “Thanks for 12 years of great music!” Basic cable provided us with “hundreds of channels and nothing worth watching,” but the cable companies hadn’t yet evolved into the rapacious apex predators we loathe.
Then the Internet happened.
Those of us who bought the first home computers remember primitive online communication through dial-up Internet Service Providers (ISP) like Prodigy, Compuserve and, of course, America Online (AOL). Who can forget the gentle sounds of your computer modem trying to connect with the AOL servers? A 14,400 baud modem gave me the blinding transmission speed of 14.4kbps to go along with my 16mHz computer clock speed. Those were the days!
But dial-up tied up one’s landline and few people could afford to spring for a second line. It was also expensive; AOL charged an hourly fee until it switched to a flat monthly rate. My 14-year old son ran up a $400 AOL bill during August 1996. (Boy, you gonna be mowing lawns until your 20s!)
Cable companies saw an opportunity and would soon pounce.
Bombastic Cable Pirates provided our cable when we moved into our house in 1998. Our Internet was still a DSL (Digital Subscriber Line) shared with a fax line. I don’t remember how much it cost, but it seemed reasonable at the time. That is, until the price jumped after the two-year introductory rate ran out. Peg was able to talk them into continuing the lower rate a couple of times, but that didn’t last. Most cable providers enjoy near-monopoly status and are only interested in hooking new customers, not retaining their existing ones.
Or, to quote Leo Getz: “They fuck you! They fuck you! They fuck you! “
We didn’t mind the price increases until they started eliminating channels, one by one, from our tier, moving them into the higher tier which cost a lot more. Complaining fell on deaf ears, as Stan and Kyle discovered when they confronted their local cable company. So, when Awesomely Terrific and Tremendous showed up in our neighborhood, promising much better customer service AND broadband Internet, we jumped – from the frying pan into the fire.
We signed up for the company’s Triple Delight package: cable, broadband internet, and switching our landline to VOIP (Voice Over Internet Protocol). The Triple Delight with Eggroll Cellular Service would have given us an additional discount, but a few years back, Awesomely offered me $600 to leave while I was working a long-term job in Nebraska. They’d assumed I’d moved there and were not pleased having to pay service fees for another company’s network every time I used my phone, even though my billing address was still in Illinois.
We were content with them for the next several years, until the inevitable price hikes started. Again, Peg managed to bargain for a lower rate a few times, but then our Internet started dropping out, first occasionally, then daily, then multiple times a day, making it completely unreliable. The modem frequently reset itself at odd times, or we had to manually reboot the system, watching that little grey circle go round and round, sometimes for several minutes. Calling Awesomely Terrific and Tremendous to complain went nowhere. “Bob” or “Dylan” or “Steve,” tech support guys with thick South Asian accents, would “run diagnostics” or fiddle with something remotely, promising resolution which never materialized.
Eventually we contacted Bombastic, which had been renamed Sempiternity (“We’re everywhere; there’s no escape!”) in January 2021. They said, “We’ll be happy to come out but you have to clear a path in the snow so we can get to the box.” Would you also like hot cocoa and cookies? They wouldn’t be able to bury the new cable until the ground thawed, so we opted to wait until fall.
A Sempiternity technician installed the new system in early November. It took him two hours to decipher the previous wiring, but he was very pleasant and thorough. He told us we might need to get one of Sempiternity’s new Wi-Fi capsules to boost our upstairs signal.
The only glitch was the need to exchange the upstairs cable box, which inexplicably turned itself off and on every ten minutes. I exchanged it at the local Sempiternity store relatively quickly and we were in business. (I had to ensure the lawn service people didn’t run over the exposed cable during their last visit of the season, but we had a relatively warm late fall, and they buried the cable before Christmas.)
When we were sure everything was working, Peg called Awesomely Terrific and Tremendous to cancel our subscription.
“We can’t cancel it today because our network is down.” Ah, the irony.
Even more ironic was the Saturday Night Live skit, airing two days later, about one man’s ordeal trying to cancel his cable subscription.
All was going well until I bought the Wi-Fi capsule. But that’s a story for the next post